
Introduction
For decades, Scotland’s history of violence has usually been explained through deprivation, alcohol, industrial decline, policing, family breakdown and wider social dislocation. Those explanations matter. But there is another factor that has rarely been given the same weight in public discussion: lead exposure.
For much of the twentieth century, lead in Scotland was not a rare environmental hazard. It was part of ordinary domestic life. It was present in old service pipes, household plumbing and lead-lined water tanks. In cities such as Glasgow and Edinburgh, soft, acidic water made the problem worse because it was highly plumbosolvent, meaning it could dissolve lead from pipework into the water people drank.
The scale of exposure was striking. In a major UK survey conducted in 1975–76, 33% of Scottish households had drinking-water lead concentrations above 50 µg/L. In Glasgow, the problem was even more acute: roughly 40% of samples exceeded 100 µg/L. These levels sit far above modern health-based expectations. This was not a niche defect in a few neglected houses. It was a widespread public health problem shaped by old homes, old plumbing, and water chemistry.
Glasgow and Edinburgh are central to this story, but in different ways. Glasgow provides one of the clearest examples of a severe citywide drinking-water lead problem. Edinburgh gives us one of the most important Scottish studies linking blood lead levels in children to behaviour. Together, they allow us to ask a difficult but important question: did Scotland’s historic lead exposure contribute, at least in part, to later patterns of violent behaviour?
This article does not argue that lead alone explains Scotland’s violent past. Crime is too complex for that. Poverty, trauma, alcohol, policing, education, inequality and neighbourhood conditions all matter. But the evidence is now strong enough to say that lead belongs inside the conversation as a serious, avoidable risk factor — one that may have left a longer social shadow than Scotland has usually acknowledged.
Table of Contents
Why Scotland Was Especially Vulnerable to Lead in Drinking Water
Scotland’s drinking-water lead problem had a particular chemistry behind it. Lead pipes are more likely to leach lead into water where the water is soft and acidic. Many Scottish supplies, especially from upland sources, had exactly those characteristics. Glasgow’s supply from Loch Katrine, for example, had a recorded pH of around 6.3 in 1976 — notably acidic and highly plumbosolvent. Where that water passed through lead pipes, lead joints or lead-lined storage tanks, the risk increased substantially.
This made Scotland unusually vulnerable. Old plumbing was already common. Older tenements and houses often retained lead service pipes, internal lead pipework or lead-lined tanks. Once lead was in contact with soft, acidic water, it could enter the household supply in significant quantities.
This was not only a technical water issue. It was also a housing issue. In older urban areas, the people most exposed were often those least able to change the plumbing. Many households were tenants, not owners. Even if a family suspected that lead was present, replacing pipes or tanks was not always within their control.
By the mid-1990s, the Scottish Office estimated that 589,000 homes in Scotland still contained lead pipes. This was not a small remnant of a vanished era. It was a live public-health problem concentrated in older urban neighbourhoods.
Glasgow’s Water Lead Problem
Glasgow is the clearest example in Scotland of a severe drinking-water lead problem. The city’s historic supply from Loch Katrine was celebrated as a great civic achievement, but the water’s chemistry created a major problem where it met lead pipes and plumbing. The water was soft and plumbosolvent, meaning it actively dissolved lead from the pipework carrying it into homes.
The numbers were serious. In 1981, 49% of sampled Glasgow households had tap-water lead at or above 10 µg/L — the World Health Organisation guideline level at the time, and a threshold now treated as a meaningful public-health concern. The significance was especially acute for infants and pregnant women. Lead in tap water could pass directly into bottle feeds. Raised maternal blood lead was also associated with tap-water lead, meaning Glasgow’s problem was not simply about old houses or regulatory breaches. It was about exposure at the most sensitive stages of human development.
Treatment measures, including lime dosing, pH correction and later orthophosphate, reduced the problem substantially. By 1993, the proportion of Glasgow households above 10 µg/L had fallen from 49% to 17%. That was a genuine public-health success.
But even after major treatment improvements, a meaningful minority of homes still exceeded guideline levels — and treatment had not replaced the pipes. Where the pipework remained, the source of exposure remained as well.
Edinburgh’s Exposure Problem
Edinburgh’s lead problem had a different evidence base, but it was just as important. The Edinburgh Lead Study, published in 1989, examined 501 children aged 6 to 9 from 18 primary schools in central Edinburgh. It measured blood lead directly — finding a geometric mean of 10.4 µg/dL in the study sample — and compared those levels with behaviour assessed using the Rutter behaviour scales, completed by both teachers and parents.
The study found that higher blood lead levels were associated with worse teacher-rated behaviour, particularly aggressive or anti-social behaviour and hyperactivity, after controlling for 30 potential confounding variables. It also found elevated indoor dust lead levels in the homes of the children studied, with a mean of 308 µg/g that increased with housing age. That points to lead paint and dust as a second exposure pathway alongside drinking water.
The later follow-up study, published in 1998, showed that water treatment and plumbing changes could reduce both household water lead and blood lead over time. But it also showed that homes without lead plumbing had far lower lead levels in their water than homes with lead pipes or lead-lined tanks. The lesson was clear: treatment can reduce exposure, but replacement deals with the source.
Why This Matters for the Crime Question
Before we even reach crime statistics, Glasgow and Edinburgh establish the first essential point: Scottish cities really did expose large numbers of people to lead through drinking water and older homes. The 1975–76 survey figures — 33% of Scottish households above 50 µg/L and roughly 40% of Glasgow samples above 100 µg/L — are not background noise. They indicate an exposure environment capable of raising blood lead levels in children to ranges now associated with measurable cognitive and behavioural impacts.
That matters because lead is not only a water-quality issue. It is a neurotoxin. It affects the developing brain, particularly the systems involved in attention, impulse control and emotional regulation. It is associated with attention problems, impulsivity, aggression, poor self-control and behavioural disruption. Those traits are also well-established risk factors for later offending, especially violent offending.
So the question is not whether lead “caused” Scottish violence in a simple way. The question is whether high early-life lead exposure may have increased the population-level risk of aggressive and impulsive behaviour in cities already under serious social strain.
That is where the lead-crime hypothesis comes in.
The Lead-Crime Hypothesis
From Public Health Concern to Crime Theory
The lead-crime hypothesis grew out of two bodies of evidence.
The first was medical and developmental: lead damages the brain, especially in early life. The second was criminological: aggressive behaviour, impulsivity, poor attention and low self-control are well-established risk factors for later offending.
The hypothesis joined these two ideas. If lead exposure damages the parts of the brain involved in attention, impulse control and emotional regulation, then widespread childhood exposure might raise the later risk of violent behaviour at population level.
The theory does not require lead to create criminals in a crude or deterministic way. Rather, it suggests that lead can push risk upward. In a city where many children are exposed, even a modest shift in behaviour and self-control could matter years later.
From Research to Public Debate
The lead-crime hypothesis moved from academic research into wider public discussion largely through Kevin Drum’s 2013 feature in Mother Jones, “America’s Real Criminal Element: Lead.” Drum did not originate the theory, but he gave it a powerful public narrative, drawing together research from public health, economics and criminology to present lead as a possible hidden driver behind the rise and fall of violent crime.
The basic argument was that violent crime rose after the postwar expansion of leaded petrol and fell after lead exposure declined — with a lag of roughly two decades, matching the time it would take exposed children to reach the peak ages for violent offending. Drum’s follow-up piece, “Lead and Crime: A Linkfest,” kept the debate alive by gathering subsequent studies, challenges and related findings.
That journalism did not settle the science, but it made the hypothesis impossible to ignore in public discussions of crime and environmental policy.
Why the Theory Caught Global Attention
The lead-crime hypothesis became compelling because it appeared across different countries and different contexts. Rick Nevin’s international work compared preschool lead exposure and later crime trends across several Western countries, including Britain, and found striking alignments. The timing of exposure changes and later crime trends matched the developmental lag expected if childhood exposure affected later behaviour.
Jessica Wolpaw Reyes strengthened the argument by using variation between US states in the speed of lead exposure reduction. Her findings supported a relationship between childhood lead exposure and later violent crime, with the strongest effect appearing in violent crime rather than property crime. That distinction matters: if lead affects impulse control and aggression specifically, we would expect the strongest link to violence rather than to opportunity-driven offending.
The Serious Version of the Theory
The serious version of the lead-crime hypothesis is not that lead explains everything. It is that lead is one important risk factor among many.
Crime rises and falls because of many forces: poverty, policing, drugs, alcohol, unemployment, inequality, school exclusion, family instability, social norms and opportunity. Lead does not replace those explanations. It sits alongside them — with biological plausibility, international evidence and Scottish behavioural evidence behind it.
What International Research Says About Lead and Violent Crime
Rick Nevin and the International Time-Series Evidence
Rick Nevin’s 2007 work gave the hypothesis its international reach. He compared preschool lead exposure with later crime trends across multiple countries and found strong associations, with the key feature being the lag: childhood exposure appeared to line up with later crime trends after enough time had passed for exposed children to reach the peak years for offending — typically around 18 to 23 years, depending on the crime category.
This was powerful because it was not confined to one city or one country. The pattern appeared across nations with different governments, policing systems and cultures. However, Nevin’s work was ecological in nature. It examined population-level trends and cannot by itself prove what happened to particular individuals. That is why subsequent work matters.
Jessica Reyes and State-Level Evidence
Jessica Reyes strengthened the argument by exploiting differences in how quickly US states reduced lead in petrol, building state-year panels with 20 to 30 year lags. Her findings supported a relationship between childhood lead exposure and later violent crime, and she found the strongest effects in violence rather than property crime.
Her later work also linked early lead exposure to childhood behaviour problems, adolescent aggression and later criminal behaviour, helping to connect the theory back to developmental pathways rather than relying only on broad historical curves.
Cohort Studies and Individual-Level Evidence
The hypothesis becomes more convincing when individual-level studies are considered. Several cohort studies have followed people from early-life lead exposure into later behavioural or criminal outcomes. These studies do not produce identical results — some show stronger effects than others — but the overall pattern supports a link between early lead exposure and later antisocial behaviour, delinquency or violence.
A systematic review by Talayero and colleagues, published in PLOS Global Public Health in 2023, concluded that diverse individual-level studies — measuring lead in blood, bone and dentine across multiple developmental windows — link early exposure to later delinquency, criminal and antisocial outcomes. The finding holds across different study designs and populations.
This does not mean every exposed child becomes violent. It means exposure can increase risk at population level.
What Meta-Analysis Adds
The most important corrective in the literature comes from meta-analysis. Higney, Hanley and Moro’s 2022 meta-analysis, drawing on 542 estimates from 24 studies, found that publication bias had inflated some earlier estimates. Their adjusted central estimates — a partial correlation of around 0.16 and an elasticity of around 0.09 — are more modest than the early claims.
Their illustrative calculations suggest that lead abatement plausibly explains around 7 to 28% of the major late-20th-century homicide decline in the United States — meaningful, but not dominant. Most of any crime decline is explained by other factors.
That is not a failure of the theory. It is a necessary correction. The better conclusion is: lead exposure appears to be a meaningful contributor to later violent crime risk, but not the primary or sole cause.
Applied cautiously to Scotland — given the limited Scotland-specific longitudinal blood-lead datasets — a reasonable evidence-consistent estimate is that lead abatement plausibly contributed on the order of 5 to 20% of Scotland’s serious-violence decline from its mid-2000s peak to its mid-2010s trough. The uncertainty is wide, and the range depends on which outcome is measured, whether homicide or broad assault, and which exposure proxy is used: petrol lead, water lead, or both combined.
The Scottish Evidence Base
What the Edinburgh Lead Study Established About Child Behaviour
The strongest direct Scottish evidence begins with the Edinburgh Lead Study, published in 1989. The researchers examined 501 children aged 6 to 9 from 18 primary schools in central Edinburgh, measured blood lead, and assessed behaviour using the Rutter behaviour scales completed by both teachers and parents. The geometric mean blood lead level in the cohort was 10.4 µg/dL.
After controlling for 30 possible confounding variables, the study found a significant relationship between blood lead and teacher-rated total behaviour problems, aggressive or anti-social behaviour, and hyperactivity. It did not find a significant relationship with the neurotic sub-score. Parent scores moved in the same direction, but did not reach statistical significance in the full model.
The paper’s plotted log-odds show a broadly linear rise across blood-lead groups, visually reinforcing the authors’ conclusion that there was a dose-response relationship with no evidence of a threshold. The authors also explain that the highest blood-lead group had about 2.4 times the odds of being in a worse behaviour category than an average child.
That matters enormously for the Scottish case. The Edinburgh study did not measure later offending, but it did identify a clear association between lead exposure and the kinds of behavioural traits that later crime research repeatedly treats as relevant to violence: aggression, impulsivity, poor self-regulation and hyperactivity. In other words, it gives Scotland a local, child-level demonstration of the behavioural pathway that the wider lead-crime literature depends on
What the Eight-Year Follow-Up Established About Water Lead and Blood Lead
The eight-year follow-up, published in 1998, added a second layer of evidence. It revisited 207 families from the original cohort, with 171 young people aged 14 to 17 providing a blood sample. The follow-up showed that household water lead fell dramatically after improvements in treatment and some removal of lead plumbing.
In homes supplied from Alnwickhill, mean water lead fell from 34.0 to 4.3 µg/L, an 87% reduction. In homes supplied from Fairmilehead, it fell from 9.3 to 3.6 µg/L, a 61% reduction. Over the same period, average blood lead fell from 11.0 µg/dL to 4.0 µg/dL. The authors were explicit that these changes reflected both water treatment and the removal of lead plumbing.
But the follow-up also showed why treatment alone was not enough. Houses with no lead plumbing had water lead levels 89% lower than houses with lead-lined tanks and 47% lower than houses with lead pipes. About one-third of households with lead tanks were still predicted to exceed the then-current 50 µg/L EC limit, and if a 10 µg/L standard were applied, 34% of households supplied from plant A and 25% from plant F would still have breached it.
The follow-up paper’s histogram makes that pattern visually clear: homes with lead tanks cluster at the highest water-lead values, while homes with no lead seen or reported are concentrated much lower down the distribution. The authors described the overall reductions in water lead and blood lead as “an important achievement in public health”, while also warning that more progress would be required if lower standards were to be met.
What Scottish Government Crime Research Says About Early-Life Lead Exposure
The Scottish evidence does not stop at public health. In its review What Works to Reduce Crime?, the Scottish Government states that early-years lead exposure has been linked to aggressive behaviour, impulsivity and ADHD, all of which are recognised risk factors for offending behaviour.
The review cites a meta-analysis of 19 studies on lead and conduct problems and notes that the association was remarkably consistent and not significantly weakened by controlling for potentially confounding factors such as home environment and social class. It also summarises the crime literature in a notably careful way: the link is most clearly established in relation to violent crime, there is less consensus on property crime, and none of the existing research claims that lead is the main cause of violent crime. Even so, the review treats lead exposure as a serious explanatory factor in variation in crime rates.
That same review is useful for another reason. Its summary model of the underlying causes of crime places low self-control near the centre of the pathway to offending. The text then explains that people with low self-control are more likely to offend and to suffer a range of other negative life outcomes. That framing matters because it matches the developmental mechanism in the lead literature almost perfectly: if lead increases impulsivity, attention problems and aggressive behaviour, then it fits naturally into the Scottish Government’s own model of how risk accumulates long before crime is officially recorded.
Emerging Scottish Research — and Why Caution Still Matters
There is also newer Scottish research that adds both depth and caution. A 2025 University of Glasgow natural experiment examined drinking-water interventions that reduced lead levels in Glasgow and Edinburgh from 1978 onwards, using administrative data on more than 650,000 births between 1975 and 2000.
The authors did not find consistent evidence that the interventions increased birthweight or reduced under-5 mortality, although they could not rule out the prevention of 1–3 deaths per thousand. Importantly, they stressed that their focus was on short-run outcomes around birth, so the findings do not rule out longer-term impacts from early-life lead exposure.
That is an important nuance. The Scottish evidence base is getting stronger, but it still does not give us a neat city-level causal estimate for later violence.
Taken together, the Scottish evidence is strongest on three points. First, lead exposure in cities such as Edinburgh and Glasgow was real, measurable and historically serious. Second, in Scotland itself, higher childhood lead burden was associated with the kinds of behavioural problems that later violence research treats as highly relevant. Third, reducing exposure through treatment and plumbing change clearly lowered both water lead and blood lead.
Where the Scottish evidence is still thinner is on the final step: the direct measurement of how far those exposure changes translated into later offending or homicide trends. So the Scottish case is already strong on mechanism, behaviour and public health, but still more cautious on direct crime attribution.
Glasgow and Edinburgh Compared
Did Glasgow Have a More Severe Drinking-Water Lead Problem Than Edinburgh?
Both Glasgow and Edinburgh sat inside the same broader Scottish risk environment: upland, low-mineral, relatively acidic water meeting old lead plumbing. Published summaries describe Glasgow as especially badly affected, with a very high share of results above 100 µg/L, although exact figures vary by survey definition and sample. Glasgow and Edinburgh were also among the first Scottish cities to begin pH-raising treatment in the late 1970s because their water was so plumbosolvent.
The published evidence is not perfectly symmetrical. Glasgow’s clearest evidence is a large household-prevalence study in the Loch Katrine supply area. Even after maximal treatment, 17% of households still had tap water lead of 10 µg/L or more in 1993, down from 49% in 1981. Tap-water lead remained the main correlate of raised maternal blood lead, and an estimated proportion of infants were exposed through bottle feeds to tap water above the WHO guideline.
Edinburgh’s strongest evidence is structured differently. The original Edinburgh Lead Study found a geometric mean child blood lead of 10.4 µg/dL in 501 children, while the eight-year follow-up showed mean household water lead falling from 34.0 to 4.3 µg/L in one supply area and from 9.3 to 3.6 µg/L in the other. Blood lead fell from 11.0 to 4.0 µg/dL. The follow-up also showed that houses with no lead plumbing had water lead levels 89% lower than houses with lead tanks and 47% lower than houses with lead pipes.
Taken together, the evidence suggests Glasgow had the broader city-scale drinking-water lead burden, while Edinburgh provides the clearest Scottish evidence of what sustained exposure did to children.
Did Glasgow Later Experience Higher Levels of Violent Crime?

If we move forward to lethal violence, the Glasgow–Edinburgh difference is stark. The official Scottish homicide table for 2003–04 to 2012–13 lists annual homicide cases for Glasgow City as 33, 39, 32, 33, 30, 24, 20, 26, 16 and 19, which sums to 272 over the decade. For the City of Edinburgh, the same table lists 6, 11, 9, 11, 11, 4, 7, 12, 7 and 2, which sums to 80.
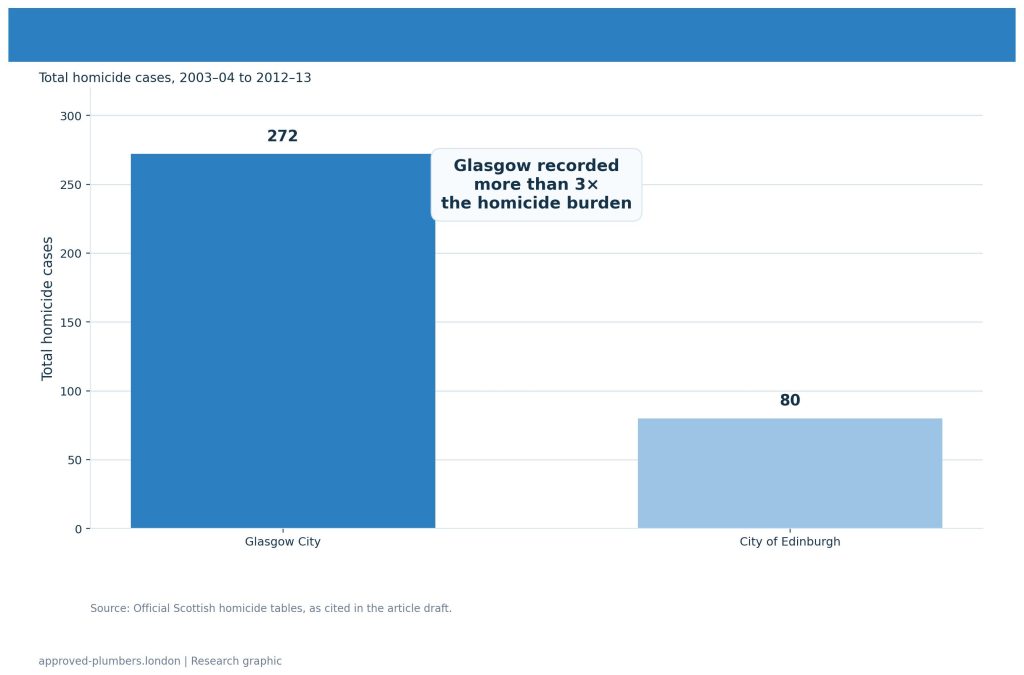
In raw counts, Glasgow therefore recorded more than three times as many homicide cases as Edinburgh across that ten-year period. These are raw counts, not population-adjusted rates, but the difference is still substantial.
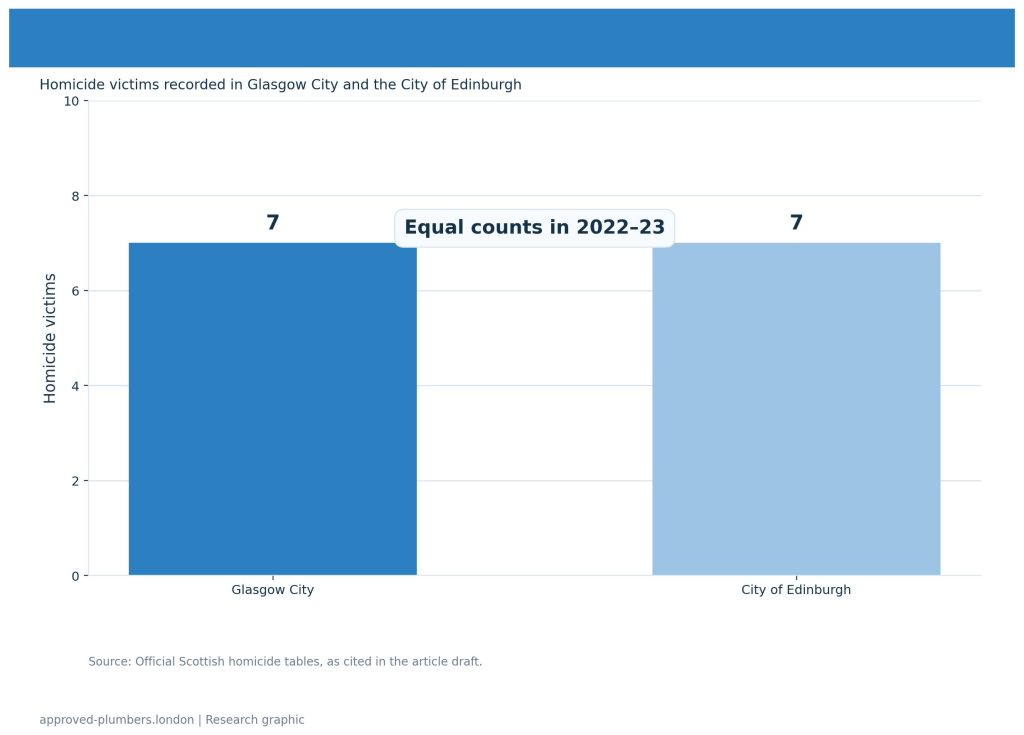
That gap narrowed dramatically later on. Official statistics for 2022–23 report that Glasgow City and the City of Edinburgh each recorded seven homicide victims.
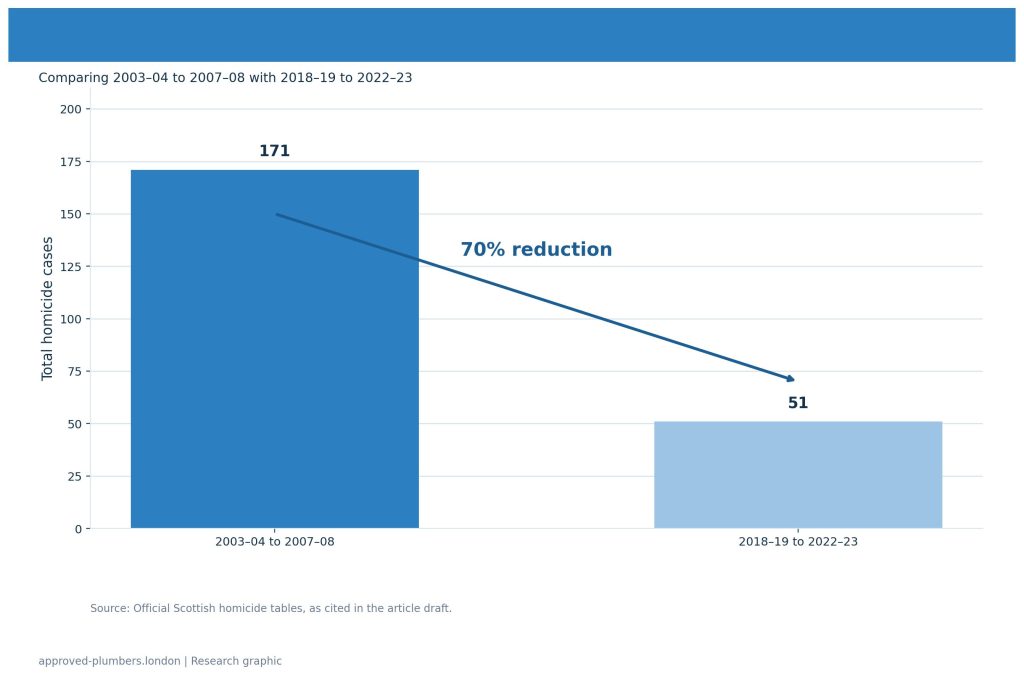
The same bulletin notes that Glasgow had 51 homicides across the five-year period from 2018–19 to 2022–23, a 70% reduction from 171 in the five-year period from 2003–04 to 2007–08..
So the contrast that once looked entrenched became much smaller over time, even though Glasgow had carried the heavier homicide burden for decades.
What the Historical Alignment Suggests — and What It Does Not Prove
Set side by side, the pattern is clearly suggestive. Glasgow has the stronger published evidence of a large, city-scale drinking-water lead burden and later showed a much heavier homicide burden. Edinburgh also had serious exposure, but its distinctive contribution is different: it produced the Edinburgh study showing that higher blood lead levels in children were associated with more aggressive, antisocial and hyperactive behaviour, even after extensive adjustment for confounders.
Those are precisely the kinds of traits the wider lead-crime literature treats as relevant to later violent offending. The Scottish Government’s own crime evidence review also links early-life lead exposure to aggression, impulsivity and ADHD, noting that the association appears strongest for violent crime.
But this is where the caution has to remain firm. The Scottish evidence base does not yet provide a published city-by-city statistical model that directly links annual drinking-water lead levels in Glasgow and Edinburgh to subsequent annual violent-crime rates. The Glasgow water studies are public-health studies. The Edinburgh papers are exposure, blood-lead and behaviour studies. The homicide bulletins are administrative crime statistics.
Put together, they create a historically plausible alignment and a strong behavioural mechanism, but not a direct quantified Glasgow-versus-Edinburgh lead-crime coefficient. The most defensible conclusion is therefore not that lead alone explains the Glasgow–Edinburgh violence gap, but that historically higher lead exposure in Glasgow may have been one important contributing factor among several.
Correlation, Causation and Caution
Why the Pattern Is Suggestive
The pattern is suggestive because several strands of evidence point in the same direction.
Scotland had unusually high drinking-water lead exposure. Edinburgh showed a link between blood lead and aggressive, anti-social and hyperactive behaviour in children. International studies link early-life lead exposure to later violent offending. Glasgow had a severe drinking-water lead problem and later a much heavier violence burden, which declined sharply from the mid-2000s.
The timing also matters. Major reductions in lead exposure occurred through a combination of drinking-water corrosion control, pipework changes and the reduction of leaded petrol. Around two decades later, Scotland’s violence trends began to shift downwards. That is broadly compatible with the 18–24 year developmental lag projected from the major exposure reductions of the 1980s and early 1990s.
That is not random noise. It is a meaningful historical alignment.
Why We Still Need Caution
Scotland’s violence decline has other strong candidate explanations that operated alongside any lead effect: recording-standard changes in the mid-2000s that affect trend interpretation; the tight entanglement of violence trends with alcohol and drug harms; concentrated deprivation in urban communities; and the active policy shift toward a public-health approach to violence prevention.
There is no single published city-by-city Scottish study directly correlating annual water-lead levels with annual violent-crime rates. The water studies are public-health studies. The Edinburgh work is a child-behaviour study. The homicide figures are administrative crime statistics. When placed together, they create a plausible and serious picture — but not direct causal proof.
Lead as a Contributing Factor
The strongest defensible position is this: lead exposure should be treated as a contributing factor in Scotland’s urban violence story, accounting plausibly for around 5 to 20% of the serious-violence decline from the mid-2000s to the mid-2010s, with significant uncertainty in that range. Most of the decline is explained by other factors.
That is more credible than overstating the case, and it fits the meta-analytic evidence better than early single-study claims. Lead may have acted as an amplifier — increasing population-level risk in cities already shaped by poverty, unemployment, housing stress, alcohol, school exclusion and policing patterns.
That is serious enough.
From Scotland’s Violence Reduction Model to London’s Lead Question
Scotland’s later success in reducing serious violence is important because it shows how the country eventually reframed the problem. The Scottish Violence Reduction Unit did not treat violence only as a law-and-order issue. It treated it as a public-health issue: something shaped by early life, poverty, inequality, despair, alcohol, trauma, peer groups and community conditions.
That shift matters for this article. A public-health approach asks what sits upstream of violence. It does not wait until harm has happened and then respond only with enforcement. It asks what can be prevented earlier, before patterns of behaviour become fixed and before young people reach crisis point.
Lead exposure belongs in that upstream conversation. It is not a replacement for the better-known explanations of violence, and it should not be used to minimise poverty, trauma, alcohol or social conditions. But it is a preventable childhood exposure linked with aggression, impulsivity, hyperactivity and poor self-control — exactly the kind of early-life risk factor that a public-health approach should take seriously.
This is where the Scottish story becomes relevant to London. London has its own serious violence problem, its own public-health response, and its own large stock of older homes where lead pipes may still be present. The lesson is not that lead explains London’s violence. That would be too crude. The lesson is that prevention must include the conditions children grow up in — including the water they drink.
Scotland’s violence reduction model tells us to look further upstream. The lead evidence tells us that old pipes and plumbing are part of that upstream environment. For older homes in London and across the Thames Water region, the practical conclusion is simple: where lead remains in the drinking-water route, it should be identified and replaced.
From Historical Exposure to Present-Day Pipe Replacement
Treatment Bought Time, but the Pipes Kept the Risk Alive
The Scottish evidence shows that treatment worked. Lime dosing, pH correction and orthophosphate reduced plumbosolvency and lowered lead levels in water across Scottish cities. Blood lead fell when exposure fell. Glasgow’s reduction from 49% to 17% of households exceeding 10 µg/L between 1981 and 1993 was a real public health success.
But the evidence also shows that treatment did not remove the source. The CREW “Lead free Scotland” report is explicit: orthophosphate dosing can reduce lead leaching, but it is not a lead-free strategy. Homes without lead plumbing consistently had far lower water lead than homes that retained lead pipes or lead-lined tanks. Treatment managed the risk. Replacement addresses the source.
The Modern Water Position
Modern water-sector strategy makes the same point. Lead found at the customer’s tap comes from lead pipes — in the communication pipe, the supply pipe or internal plumbing — not from the treatment works. Orthophosphate dosing provides a protective passivating layer inside pipes, but it does not replace them. That is why long-term lead strategy increasingly points toward pipe replacement. Treatment is a mitigation. Replacement is the durable answer.
The Responsibility Problem
One reason the problem persists is the question of responsibility. The water company is usually responsible for the communication pipe, normally up to the property boundary or outside stop tap. The property owner is usually responsible for the private supply pipe and internal plumbing beyond that point.
That split matters. A water company can replace its side, but if lead remains on the customer side, the drinking-water route still includes lead. Full protection depends on addressing both sides of the supply route.
This is why clear public information is essential. Many homeowners do not know where responsibility changes, what pipe material they have, or how to begin the replacement process. The Scottish experience — where a grant mechanism existed for replacing lead pipes where tests exceeded threshold values — shows that public support and clear guidance can accelerate replacement when the will exists.
Why Older Homes Still Matter
The risk is not evenly distributed. It is more likely in older homes, especially where the incoming supply or internal plumbing has never been modernised. Housing age is not proof of lead pipes, but it is the most consistent first indicator of where checks should begin. In London, where a large share of homes predate the period when lead pipework was removed from normal use, that indicator still covers a significant portion of the housing stock.
Old pipework can continue to shape exposure long after public attention has moved on. The families living in older homes today should not have to rely on guesswork.
Conclusion
Lead does not explain Scotland’s violent past on its own. The evidence is too careful, and the history is too complex, for that kind of claim. Poverty, trauma, inequality, alcohol, policing, family instability and neighbourhood conditions all remain central to any serious account of violence.
But the Scottish record is now strong enough to support a more measured and specific conclusion: lead exposure belongs inside that history as a serious, avoidable risk factor, plausibly contributing around 5 to 20% of Scotland’s major serious-violence decline from the mid-2000s to the mid-2010s. The uncertainty in that range is real, and most of the decline is explained by other causes. But the contribution of lead reduction is consistent with the available evidence and should not be dismissed.
In Edinburgh, higher childhood blood lead was associated with worse behaviour — particularly aggression, anti-social behaviour and hyperactivity. In Glasgow, historic drinking-water lead exposure was severe and widespread: 49% of sampled households above 10 µg/L in 1981, reduced to 17% by 1993 through treatment, but not eliminated while lead pipes remained. International research supports the idea that early lead exposure can contribute to later violent offending, particularly through its effects on impulse control, aggression and behaviour. And the timing of Scotland’s violence decline — peaking around 2006–07 and falling through the mid-2010s — aligns with the 18–24 year developmental lag projected from the major exposure reductions of the 1980s and early 1990s.
The lasting lesson is larger than crime alone. Scotland’s experience shows how old pipes and plumbing can cast a long social shadow: first through exposure, then through effects on child development and behaviour, and finally through risks that can echo across communities for generations.
Even if lead explains only part of Scotland’s violence story, it still represents avoidable harm on a generational scale. Treatment reduced risk, but it did not end the source.
The durable public-health answer remains clear: replace the lead.
Sources
- House of Commons Library (1997). Lead in Drinking Water (Research Paper 97/65). Key Scotland figures on 1975–76 household water-lead distribution and Scottish lead-pipe prevalence; UK petrol lead policy timing.
- CREW – Scotland’s Centre of Expertise for Waters (2016). Lead free Scotland — final report and annex. Scottish study summaries, Glasgow maternal blood lead survey, corrosion control context and residual risk discussion.
- Thomson, G.O.B. et al. (1989). “Blood-Lead Levels and Children’s Behaviour — Results from the Edinburgh Lead Study.” Journal of Child Psychology and Psychiatry, 30(4), 515–528.
- Macintyre, S. et al. (1998). “Changes in blood lead and water lead in Edinburgh: An eight year follow-up to the Edinburgh Lead Study.” Journal of Epidemiology and Community Health, 52(6), 427–428.
- Scottish Government (2014). What Works to Reduce Crime? A Summary of the Evidence.
- Scottish Government homicide statistics / official homicide tables.
- Scottish Centre for Crime and Justice Research (2024). Policy briefing on violence trends in Scotland — non-sexual violence time series and Glasgow patterns.
- BMC Public Health (2021). Long-run homicide pattern in Scotland and concentration in deprived Glasgow areas. DOI: 10.1186/s12889-021-11167-z.
- University of Glasgow (2025). Natural experiment examining drinking-water interventions and early-life outcomes in Glasgow and Edinburgh.
- Rick Nevin (2007). “Understanding international crime trends: The legacy of preschool lead exposure.” Environmental Research, 104(3), 315–336. DOI: 10.1016/j.envres.2007.02.008.
- Jessica Wolpaw Reyes (2007). “Environmental Policy as Social Policy? The Impact of Childhood Lead Exposure on Crime.” NBER Working Paper 13097. DOI: 10.3386/w13097.
- Higney, A., Hanley, N. & Moro, M. (2022). “The lead-crime hypothesis: A meta-analysis.” Regional Science and Urban Economics, 97, 103826. DOI: 10.1016/j.regsciurbeco.2022.103826.
- Talayero, M.J. et al. (2023). “The association between lead exposure and crime: A systematic review.” PLOS Global Public Health, 3(8): e0002177. DOI: 10.1371/journal.pgph.0002177.
- Thames Water, water quality lead strategy and lead pipe replacement investment documents.
