Executive summary
The overall body of evidence supports an association between childhood lead exposure and ADHD diagnosis and/or ADHD-related symptom domains. The most consistent links are with hyperactivity, impulsivity, and broader externalising behavioural dysregulation. That does not mean lead is the sole cause of ADHD. It does mean lead is a serious and preventable neurodevelopmental risk factor that remains relevant even at exposure levels once regarded as too low to matter. [1–7]
Recent quantitative syntheses strengthen that conclusion. A 2024 meta-analysis reported a significant association between childhood lead exposure and ADHD development, while a separate meta-analysis of cohort studies found increased ADHD risk in higher-exposure groups. Prospective evidence is especially important because it helps address temporality. In the Boston Birth Cohort, early-childhood blood lead levels of 5 to 10 µg/dL were associated with higher odds of physician-diagnosed ADHD, with a stronger association in boys. Other studies suggest that behavioural effects may be detectable even at lower levels. In a Mexico City cohort with a mean blood lead level of about 3.4 µg/dL, segmented models identified positive associations between lead and hyperactivity/impulsivity scores in the ≤5 µg/dL range. [6–9]
UK public-health and toxicology sources support the same low-threshold interpretation. WHO states that no level of lead exposure is known to be without harmful effects, and its childhood lead poisoning guidance identifies neurodevelopmental, behavioural and attention-related effects in children. Public Health England described lead as a non-threshold contaminant, found strong evidence of adverse cognitive effects below 5 µg/dL, found evidence of externalising behaviours including attention, impulsivity and hyperactivity below 10 µg/dL, and recommended lowering the intervention concentration for children and pregnant women. That recommendation was implemented: the public-health intervention concentration in England was lowered from 10 µg/dL to 5 µg/dL for children under 16 and pregnant women, with effect from 5 July 2021. [1–5]
The practical implication is sharper in infancy. WHO identifies drinking-water systems with lead solder and lead pipes as sources of childhood exposure, and notes that infant formula and the water used to prepare infant foods may contain lead. NHS guidance says powdered formula should be made up with fresh water from the cold tap, while the Drinking Water Inspectorate states that homes built before 1970 may still have lead pipework if they have not been modernised. In older homes, formula feeds made with tap water can therefore create a direct and repeated exposure pathway at the stage of life when the developing brain is most vulnerable. [1,14,15]
This article makes four core points. First, lead exposure should be understood as a probable causal contributor to ADHD risk and/or ADHD-like symptom burden, especially hyperactivity and impulsivity. Second, low-level exposure remains clinically and publicly important; the absence of overt poisoning does not imply the absence of neurodevelopmental harm. Third, because exposure in older housing can arise through legacy plumbing, paint, dust and soil, prevention must prioritise source identification and removal rather than reassurance alone. Fourth, in London, this question remains relevant because older housing, historic plumbing and ongoing lead pipe replacement programmes are still part of the water-quality landscape. [1–5,13,15,16]
Table of Contents
Scope, definitions, and approach
This article examines the relationship between lead exposure and ADHD diagnosis and symptom domains, with particular attention to hyperactivity, impulsivity, attention problems and related behavioural dysregulation. It draws on systematic reviews, meta-analyses, key cohort and behavioural studies, UK public-health guidance, and water-industry material relevant to lead exposure in older housing. [2,6–10,13–16]
A distinction that must remain explicit throughout is the difference between blood lead and water lead. Blood lead concentration is measured in µg/dL and is used as a biomarker of exposure. Lead in drinking water is measured in µg/L and is regulated at the tap. These are not interchangeable units. Public Health England’s intervention review concerns blood lead in children and pregnant women, while drinking-water regulation concerns the concentration of lead in water supplied at the consumer tap. [2–4,15,16]
The exposure literature uses several related constructs. Blood lead level is the most common biomarker and is usually treated as a measure of relatively recent exposure. Bone lead is sometimes used as a cumulative exposure marker because lead can remain stored in calcified tissue for years. Prenatal exposure is usually inferred from maternal blood lead, cord blood, maternal bone lead mobilisation or related biomarkers, and remains especially important because lead can cross the placenta and expose the developing fetus. [1,5,11]
ADHD-related outcomes also vary across studies. Some use physician diagnosis or health records, which offer stronger clinical specificity. Others use validated behavioural rating scales, teacher ratings, parent reports or symptom subdomains. This distinction matters because the evidence is more consistent for hyperactivity, impulsivity and externalising behavioural effects than for all ADHD domains equally. [6–11]
Because this article is concerned with practical exposure pathways, it also links the research evidence to older homes and legacy plumbing. WHO identifies drinking water delivered through lead pipes, solder and fittings as a possible exposure source. Public Health England identifies drinking water, flaking paint, contaminated soil, food and imported products as ongoing sources of exposure. Thames Water states that lead found at customers’ taps may come from lead pipework rather than water leaving treatment works, and the Drinking Water Inspectorate states that many older properties built before 1970 may still have lead pipework if they have not been modernised. [1,2,15,16]
Evidence synthesis from systematic reviews, meta-analyses, and major studies
The overall evidence base supports an association between childhood lead exposure and ADHD diagnosis and/or ADHD-related symptom domains. The signal is strongest not for every ADHD feature equally, but for hyperactivity, impulsivity and broader externalising behavioural dysregulation. That distinction matters. It allows the evidence to be stated more precisely: lead should be understood not as a simple one-factor explanation for ADHD, but as a serious and preventable neurodevelopmental risk factor with consistent links to clinically relevant behavioural traits. [2,6–11]
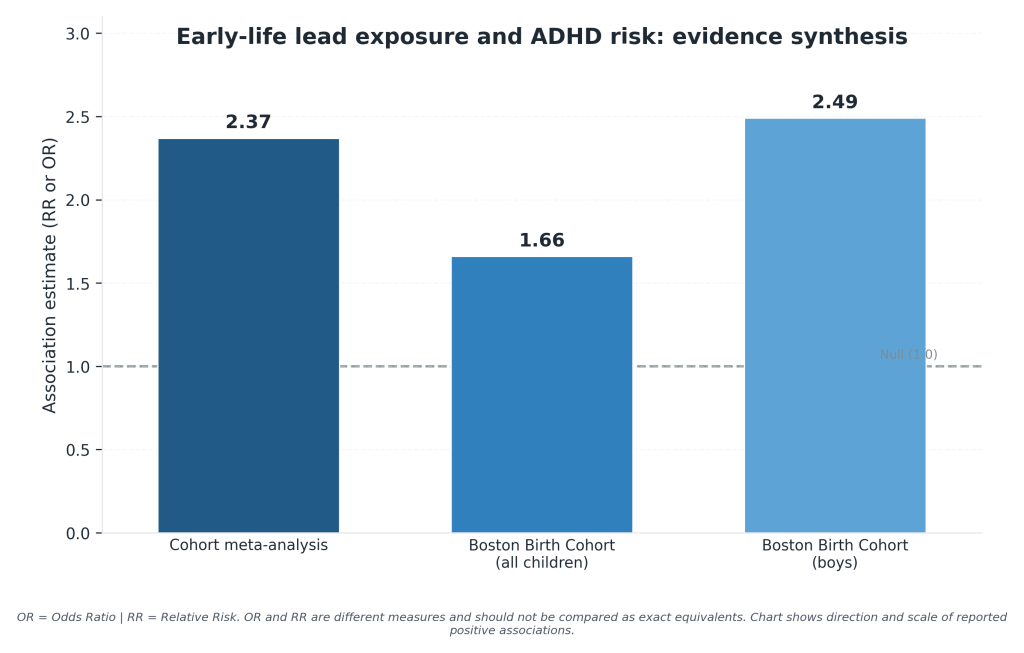
Recent quantitative syntheses strengthen the case that the association is real rather than incidental. A 2024 meta-analysis identified 14 studies with a final pooled sample of 7,618 participants, including 2,554 ADHD cases, and reported that childhood lead exposure was significantly associated with a higher risk of ADHD development. A separate 2022 meta-analysis of cohort studies found that children exposed to higher levels of lead were at greater risk of developing ADHD than children exposed to lower levels, with a pooled risk ratio of 2.37 and moderate heterogeneity. [6,7]
The strongest single studies are the ones that establish temporality. In the Boston Birth Cohort, researchers analysed 1,479 mother–child pairs and found that early-childhood blood lead levels of 5 to 10 µg/dL were associated with a 66% increased risk of physician-diagnosed ADHD. Among boys, the association was substantially stronger. This is important because lead exposure was measured before ADHD diagnosis, which materially strengthens causal interpretation compared with purely cross-sectional symptom studies. [8]
Evidence at lower exposure levels is just as important, because modern public-health practice no longer treats 10 µg/dL as the meaningful boundary. In a Mexican study of 578 children aged 6 to 13 years, the mean blood lead level was only 3.4 ± 2.9 µg/dL. Yet even at that range, adjusted segmented models found that a 1-µg/dL increase in blood lead was positively associated with hyperactivity and restless-impulsivity scores, but only in children with blood lead levels at or below 5 µg/dL. The study did not find the same pattern for inattentive symptoms, which again points to a more specific behavioural profile rather than a generic claim that all ADHD domains are equally affected. [9]
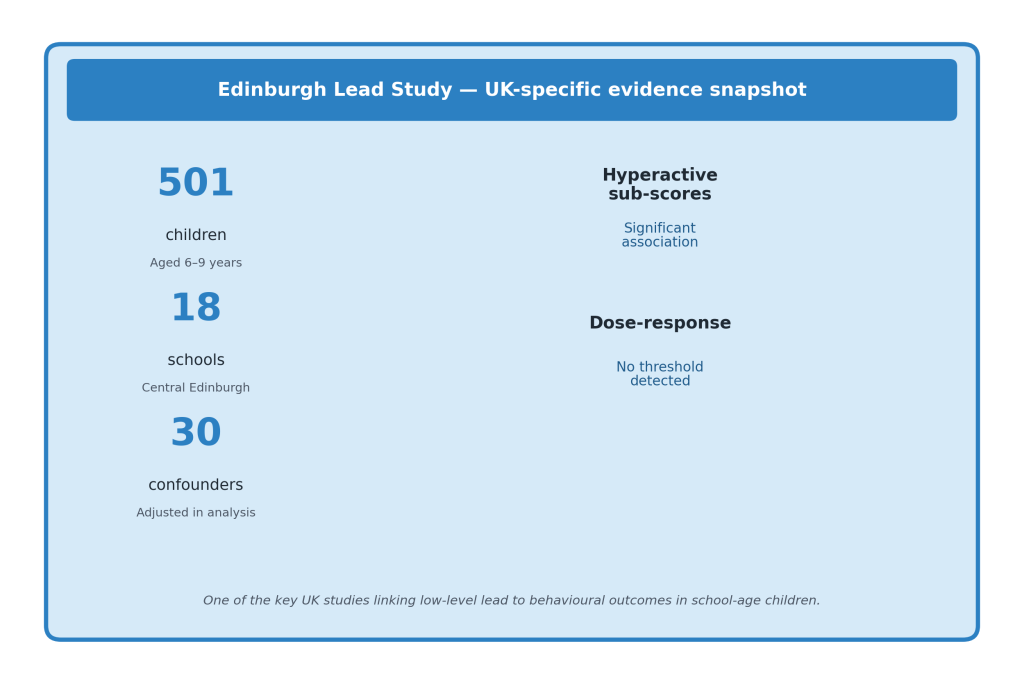
The most important UK-specific behavioural study remains the Edinburgh Lead Study. In a sub-sample of 501 boys and girls aged 6 to 9 from 18 primary schools in central Edinburgh, higher blood lead was significantly associated with teachers’ ratings of total behaviour problems and specifically with aggressive/anti-social and hyperactive sub-scores, even after taking 30 possible confounding variables into account. The authors also reported a dose-response relationship with no evidence of a threshold. [10]
Public Health England’s later review points in the same direction by concluding that there is strong evidence for adverse cognitive effects below 5 µg/dL and evidence of externalising behaviours, including attention, impulsivity and hyperactivity, below 10 µg/dL. That matters because the behavioural literature and the UK public-health interpretation are not pulling in different directions. Both support the conclusion that low-level lead exposure can be developmentally meaningful. [2]
Taken as a whole, the literature supports four conclusions. First, childhood lead exposure is associated with ADHD diagnosis and with ADHD-related symptom domains. Second, the association is most consistent for hyperactivity, impulsivity and related externalising behaviours rather than for every symptom dimension equally. Third, the effects are not restricted to historically high blood lead concentrations; low-level exposure still matters. Fourth, the public-health implication is preventive rather than merely diagnostic: the absence of obvious poisoning does not imply the absence of developmental harm. [1–11]
Dose–response, thresholds, and evidence at low-level exposure
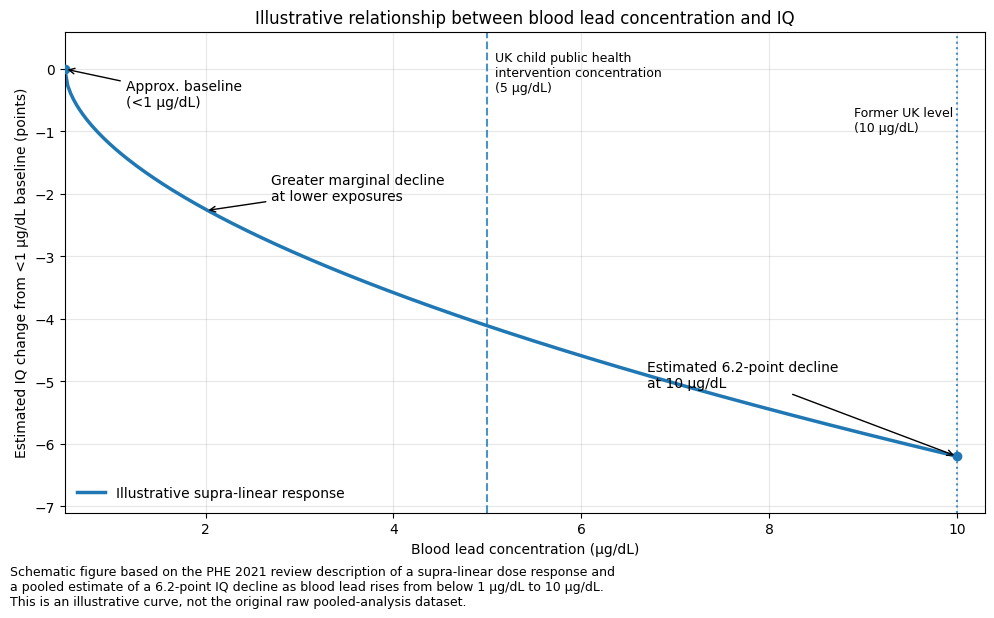
The central point is that lead does not behave like a toxicant with a clearly safe floor below which developmental harm can be ruled out. Public Health England’s 2021 review describes lead as a non-threshold contaminant and concludes that adverse effects may occur at any exposure, even though operational thresholds are still needed for surveillance and intervention. WHO’s public-health guidance makes the same point directly: there is no level of exposure to lead that is known to be without harmful effects. [1,2,5]
That is why dose–response matters more than the old language of “safe” versus “unsafe.” The evidence reviewed by Public Health England shows a supra-linear or steeper-at-the-bottom relationship for intelligence-related outcomes. One pooled analysis found an estimated decline of 6.2 IQ points as blood lead rose from <1 µg/dL to 10 µg/dL, with proportionally greater harm from the initial lower-level increases than from later increases at higher concentrations. [2,12]
This matters just as much for behaviour as it does for IQ. Public Health England’s review concludes that there is strong evidence for adverse effects on cognitive function at blood lead concentrations below 5 µg/dL, and evidence of externalising behaviours — attention, impulsivity and hyperactivity — below 10 µg/dL. In the Mexican child cohort study, mean blood lead was only 3.4 µg/dL, yet adjusted models found that a 1-µg/dL increase in blood lead was positively associated with hyperactivity and restless-impulsivity scores in children whose blood lead was ≤5 µg/dL. [2,9]
The prospective ADHD evidence points in the same direction. In the Boston Birth Cohort, children with early-childhood blood lead levels of 5 to 10 µg/dL had a 66% increased risk of physician-diagnosed ADHD, and the association was stronger in boys. Read alongside the Mexican low-level symptom data and the Edinburgh Lead Study’s finding of a dose-response relationship with hyperactive sub-scores and no evidence of a threshold, the pattern is difficult to dismiss as an artefact of outdated high-exposure settings. [8–10]
For the purposes of this article, “low-level exposure” should not be mistaken for “low-risk exposure.” It refers to blood lead concentrations below older intervention cut-offs, not to exposure that can safely be ignored. That distinction is especially important when the discussion turns to exposure pathways in older housing. If relatively small increases in blood lead can produce proportionally meaningful harm at the lower end of the dose–response curve, then repeated ingestion from lead-containing plumbing becomes more concerning, not less — especially for unborn babies, infants and young children, whose developing brains are the most vulnerable. [1,2,5,12,15,16]
Public-health interpretation and intervention thresholds
Public-health guidance on lead has moved in one clear direction: intervention thresholds have been lowered, but they are not treated as safety thresholds. WHO states that there is no level of lead exposure known to be without harmful effects. Public Health England reached the same practical conclusion in its 2021 review, describing lead as a non-threshold contaminant and concluding that harm may occur from any exposure, even though operational concentrations are still needed to trigger surveillance and case management. [1,2,5]
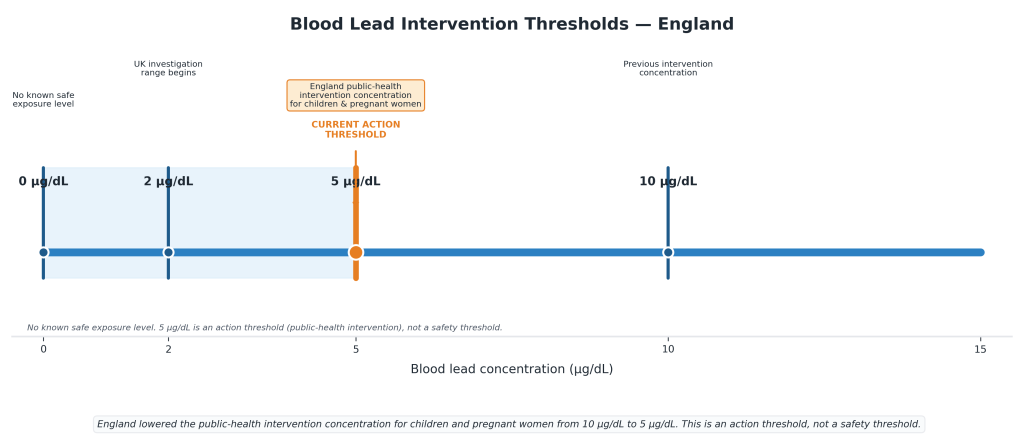
This distinction is essential. A blood lead intervention concentration is an action point, not a dividing line between “safe” and “unsafe.” In England, the public-health intervention concentration for children under 16 and pregnant women was lowered from 10 µg/dL (0.48 µmol/L) to 5 µg/dL (0.24 µmol/L), with effect from 5 July 2021. Current UKHSA guidance states that at concentrations at or greater than 5 µg/dL, UKHSA should be informed in England and clinical and environmental monitoring should begin, with systematic identification of potential sources and other vulnerable individuals. Concentrations above 2 µg/dL and below 5 µg/dL are also widely accepted in the UK as a range above which investigation should occur and a source should be identified. [2–4]
A second distinction must also be kept clear throughout: blood lead and lead in drinking water are measured in different units and operate under different regulatory logics. Blood lead concentration is measured in µg/dL and is used as a biomarker of exposure. Lead in drinking water is measured in µg/L and is regulated at the tap. In England, the regulatory limit for lead in drinking water remains 10 µg/L, while public-health intervention for blood lead in children and pregnant women now operates at 5 µg/dL. [2–4,15,16]
This matters because a legal drinking-water limit is not the same thing as a safe biological threshold. Lead measured in water is only one contributor to blood lead, and blood lead reflects total exposure across routes: water, paint, dust, soil, food, imported products and other sources. Repeated ingestion from legacy plumbing can still be clinically and developmentally important, especially when the exposure involves infants, pregnant women or young children. [1–5,13,15,16]
Taken together, the public-health interpretation is straightforward. First, there is no safe blood lead threshold for children. Second, 5 µg/dL is the current operational threshold for public-health intervention in children and pregnant women in England, not a declaration of safety below that point. Third, the drinking-water limit of 10 µg/L should not be confused with a safe biological threshold. Finally, because the evidence base points toward harm at low concentrations and because the most vulnerable groups are unborn babies, infants and young children, the logical emphasis of policy is prevention: identify the source, remove the exposure, and do not confuse regulatory action points with biological harmlessness. [1–5,15,16]
Bottle-fed infants, drinking water, and why older homes matter
Bottle-fed infants deserve particular attention because drinking water can become a direct and repeated route of lead ingestion. Current NHS guidance says powdered infant formula should be made up using fresh water from the cold tap, and that bottled water is not recommended for making up a feed. That means any lead present in domestic plumbing or the incoming supply can move into the bottle during ordinary daily feeding. [14]
WHO’s childhood lead guidance supports the significance of that pathway. It identifies drinking water delivered through lead pipes, solder and fittings as a possible source of exposure. WHO also notes that lead stored in bone can be released into blood during pregnancy, becoming a source of exposure to the developing fetus. [1,5]
This route matters because infants are among the groups most vulnerable to lead’s neurodevelopmental effects. Lead can affect the developing brain and central nervous system, and children absorb more lead than adults from an ingested dose. Public Health England similarly concludes that lead exposure is especially harmful in young children and the developing fetus, and that a precautionary approach to minimising in utero exposure is consistent with the evidence. [1,2,5]
In the UK, the practical source of lead in drinking water is usually not the treatment works or the wider mains supply, but historic pipework in and around older properties. The Drinking Water Inspectorate states that before 1970, lead pipework was commonly used to connect properties to the mains water network, that many older properties which have not been modernised may still have lead pipework, and that lead dissolves into water while it stands in the pipe. It also states that infants, including unborn babies, and children are particularly at risk because lead can adversely affect mental development and may be a factor in behavioural problems. [15]
Thames Water’s public guidance says its water mains are not made of lead, that there is virtually no lead in drinking water leaving treatment works, and that homes built after 1970 are unlikely to have lead pipes. However, it also states that older properties may have lead pipes feeding the property or in internal plumbing, and that small amounts of lead may dissolve into the water where such pipework is present. [16]
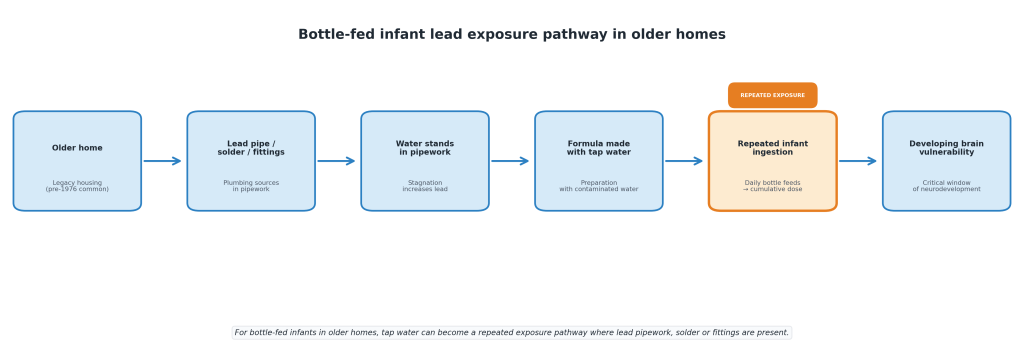
The implication is straightforward. For bottle-fed infants in older homes, lead in tap water is not a theoretical or secondary route of exposure. It is a plausible, repeated ingestion pathway at the precise stage of life when the brain is developing fastest and is least protected from toxic insult. In that setting, the central public-health task is not reassurance alone. It is to identify whether lead pipes, solder or fittings are present, assess the exposure properly, and remove the source wherever possible. [1,2,14–16]
One boundary should be stated plainly. The exposure pathway described here is documented: NHS guidance directs that formula be made up with fresh water from the cold tap, WHO identifies water used to prepare infant feeds as a source of lead, and the Drinking Water Inspectorate confirms that properties built before 1970 may retain lead pipework. What does not exist is a study measuring ADHD or behavioural outcomes in bottle-fed infants stratified by the lead content of the water used to prepare their feeds. The case for attention here rests on combining an established exposure route with an established developmental risk factor, not on outcome evidence specific to this group. That is a sound basis for prevention. It is not the same as a finding, and should not be read as one. [1,14–16]
Older homes, legacy plumbing, and London relevance
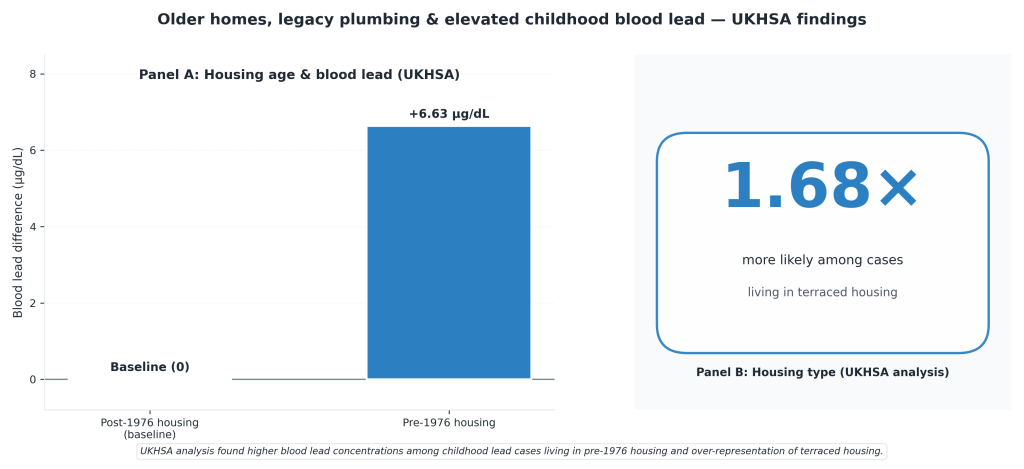
The relevance of older housing is not speculative. A 2022 UKHSA retrospective cohort study of childhood lead cases in England found that, after adjustment, cases living in housing built before 1976 had blood lead concentrations 0.32 µmol/L — equivalent to 6.63 µg/dL — higher than cases in post-1976 housing. It also found that cases were 1.68 times more likely to be living in terraced housing than other children nationally. The authors concluded that housing age and type can act as proxies for lead exposure risk through lead-contaminated paint, leaded water supply pipes and contaminated dust. [13]
That does not mean the age of a property proves that lead is present in any specific home. It means older housing makes legacy exposure sources more plausible. Public Health England’s review identifies flaking or chipped lead paint and lead paint dust as major sources of exposure in children and says lead paint may still be present in properties built before the 1960s. The same report also identifies drinking water where historic lead piping, soldering or fittings are present in the home or at service connections as an ongoing source of exposure. [2]
For London, the relevance is reinforced by Thames Water’s operational and public-facing material. Its lead guidance states that properties built before 1970 may have lead pipes, that the company’s water mains are not made of lead, and that there is virtually no lead in drinking water leaving treatment works. Its lead pipe replacement scheme also distinguishes between customer-owned supply pipework and Thames Water-owned communication pipework, making clear that responsibility for removing the exposure pathway is split between the property owner and the water company. [16]
Thames Water’s long-term water-quality enhancement case sets out the scale of the issue more directly. It describes lead pipework in contact with drinking water as a public-health risk, proposes replacement of 54,000 lead communication pipes in the 2025–2030 period, and frames the long-term solution around removing lead pipework rather than relying indefinitely on mitigation alone. It also notes the need to support customer-side pipe replacement, because replacing only the utility side does not necessarily remove exposure at the tap. [17]
The correct conclusion, then, is not that every older London property contains lead plumbing, nor that housing age alone proves exposure. It is that older homes remain one of the most credible and useful indicators of lead risk because they concentrate the exact hazards identified across the evidence base: old paint, old service pipes, old solder and contaminated dust. In a city where the water utility is still planning multi-AMP lead pipe replacement through to 2050, London relevance is built into the problem itself. [2,13,15–17]
Mechanisms and causal interpretation
The biological plausibility of lead as a contributor to ADHD-related outcomes is strong. Lead is a developmental neurotoxicant. It can affect the developing brain and central nervous system, and WHO states that children are particularly vulnerable because they absorb more lead than adults from an ingested dose and because frequent hand-to-mouth behaviour increases exposure to contaminated dust, soil and paint. [1,5]
That mechanistic account fits the human epidemiology. The behavioural signal in the literature clusters around domains that depend heavily on cognitive control, behavioural regulation and executive function. In the Mexican child study, low-level blood lead exposure was positively associated with hyperactive/impulsive behaviours but not inattentiveness, suggesting that lead may exert a more specific effect on behavioural regulation than on all ADHD symptom domains equally. Nigg and colleagues reached a similar conclusion in a clinically diagnosed ADHD sample, finding that low blood lead levels were associated with hyperactivity-impulsivity rather than inattention-disorganisation, and that the effect appeared to be mediated by weak cognitive control. [9,11]
The toxicokinetics also support a causal reading rather than a coincidental one. WHO states that lead is stored in teeth and bones, where it can accumulate over time, and that lead stored in bone can be released into blood during pregnancy, exposing the fetus. Public Health England’s review is consistent with this, concluding that there is strong evidence for adverse cognitive effects at blood lead concentrations below 5 µg/dL, and evidence of externalising behaviours including attention, impulsivity and hyperactivity below 10 µg/dL. [1,2,5]
A causal interpretation is further strengthened by the pattern of evidence across study designs. The Boston Birth Cohort is especially important because blood lead was measured in early childhood before ADHD diagnosis. That prospective sequencing matters because it helps address one of the main objections to the literature: reverse causation. The concern is real — children with developmental conditions or pica-like behaviour may ingest more dust, paint flakes or soil — but prospective evidence shows that lead exposure can precede the behavioural outcome, not just follow it. [8,13]
The remaining caution is that lead is not specific to ADHD. It affects multiple organ systems, and childhood lead exposure is socially patterned: poorer housing, old paint, historic plumbing, contaminated dust, nutritional deficiency and psychosocial stress often travel together. That means no serious reading of the evidence should claim that lead explains all ADHD or even most ADHD. But specificity is not the right test for a multisystem developmental toxicant. The better judgement is narrower and stronger: lead exposure is a biologically plausible, temporally credible, dose-relevant and preventable contributor to ADHD risk and ADHD-like symptom burden, especially in the domains of hyperactivity, impulsivity and behavioural dysregulation. [1–13]
Limitations and research gaps
The evidence base is strong enough to justify concern, but it is not methodologically neat. Most of the human literature linking lead exposure to ADHD and related behavioural outcomes is observational, which means residual confounding remains a live issue. Lead exposure tends to cluster with older housing, poorer environmental conditions, nutritional disadvantage, parental occupational exposures, contaminated dust and soil, and wider socioeconomic inequality. Public Health England notes that the health effects of low-level lead exposure are likely to be more severe in the context of existing socioeconomic and health inequalities, while the UKHSA housing study acknowledges that important exposures such as diet, soil, consumer products and other environmental sources could not be fully captured in its models. [2,13]
A second limitation is exposure measurement. Much of the epidemiological literature relies on a single blood lead measurement, even though exposure may fluctuate over time and a single result may not fully represent the child’s cumulative neurodevelopmental burden. This matters especially when the outcomes of interest may reflect exposure across sensitive windows rather than at a single moment. WHO’s guidance also makes clear that lead can accumulate in bone and be released during pregnancy, which means both timing and route of exposure are more complex than a single postnatal blood lead value can capture. [1,5]
A third problem is outcome heterogeneity. Some studies use physician-diagnosed ADHD, others use symptom scales, teacher ratings, parent reports or broader externalising behaviour constructs. That makes the literature harder to synthesise cleanly and partly explains why the signal is stronger for some domains — especially hyperactivity, impulsivity and behavioural dysregulation — than for every ADHD subtype equally. Public Health England’s own review reflects this by distinguishing between stronger evidence for cognitive effects below 5 µg/dL and evidence for externalising behaviours below 10 µg/dL. [2,6–10]
There are also important UK data gaps. Public Health England states that there have been no recent representative blood lead estimates in children in England, and the UKHSA housing paper similarly notes the absence of recent comprehensive survey data estimating how many children in England are exposed to lead. That matters because it limits any attempt to calculate a precise contemporary UK population relationship between blood lead exposure and later ADHD diagnosis. The same UKHSA paper also notes that passive surveillance systems are likely to capture the more severe end of the case spectrum. [2,13]
These gaps point to a clear research agenda. England needs updated, representative child biomonitoring data; better linkage between blood lead concentrations and neurodevelopmental outcomes; repeated measurements rather than one-off tests; more precise distinction between prenatal, infant and later-childhood exposure windows; and stronger environmental source confirmation, especially where lead pipes, solder, fittings, paint or dust are suspected. The absence of perfect evidence is not a reason to relax prevention: when lead is a non-threshold contaminant, the central public-health task remains the same — reduce exposure at source. [1,2,13]
Public-health and remediation implications
The implications of the evidence are preventive rather than merely diagnostic. Public Health England’s review concludes that lead is a non-threshold contaminant and that only primary prevention of any exposure will prevent harm altogether. It is explicit that even children with blood lead concentrations below 5 µg/dL may still experience adverse effects, which means intervention thresholds must be understood as action points, not safety lines. WHO takes the same position: the harmful impacts of lead exposure are entirely preventable. [1,2,5]
For public-health practice, that means a child with raised blood lead should trigger source identification and pathway interruption, not reassurance alone. The UKHSA housing study states that timely removal or abatement of the exposure source, or interruption of the exposure pathway, is the mainstay of case management. It concludes that public-health action should target families more at risk in older housing by raising awareness of the potential presence of lead pipes and lead paint, and that interventions should involve wider stakeholders including housing and environmental professionals, the private sector, and parents and carers. [13]
In practical terms, remediation has to focus on the environments where exposure is still most plausible. Public Health England identifies flaking or chipped lead paint and lead paint dust as major sources of exposure in children with elevated blood lead concentrations. The same report also identifies drinking water where historic lead piping, soldering or fittings are present in the home or at service connections, along with contaminated soil, food, imported cookware, toys, spices, cosmetics and traditional medicines. WHO identifies drinking water through lead pipes, solder and fittings as a possible exposure source. [1,2,5]
For drinking water specifically, remediation must distinguish between short-term exposure reduction and long-term source removal. The Drinking Water Inspectorate advises running the tap to clear water that has been standing in lead pipework as a short-term measure, but states that if lead pipes or another lead source are present, they should be replaced as soon as possible. Thames Water similarly recommends replacing lead pipework through its lead replacement scheme where possible. [15,16]
This is also why remediation cannot be treated as a water-company-only issue. Thames Water’s lead pipe replacement scheme makes clear that the customer owns the internal pipework and supply pipe, while Thames Water owns the communication pipe. That split makes complete public-health protection harder to deliver, because replacing only the utility side does not necessarily remove the exposure at the tap. Thames Water’s long-term enhancement case therefore proposes not just communication-pipe replacement, but also customer trials, education, financial support and partnership working to support customer-side removal. [16,17]
The strongest public-health implication is simple. Lead exposure in children should be treated as a source-removal problem. Where lead is suspected, especially in older housing or in homes with babies, young children or pregnant women, the priority should be to identify whether exposure is coming from paint, dust, soil, plumbing or imported products, and to remove that source wherever possible. That approach is consistent with WHO’s prevention model, Public Health England’s non-threshold interpretation, the UKHSA housing study’s recommendations, DWI advice, and Thames Water’s conclusion that durable drinking-water risk reduction depends on replacing the pipework that creates the exposure. [1,2,5,13,15–17]
Conclusion
Lead exposure does not need to be the sole cause of ADHD to matter. The evidence supports a more precise and more useful conclusion: lead is a preventable neurodevelopmental risk factor associated with ADHD diagnosis and with ADHD-related behavioural domains, particularly hyperactivity, impulsivity and externalising dysregulation. The evidence is strongest when read across several layers at once: meta-analysis, prospective birth-cohort evidence, low-level symptom studies, the Edinburgh Lead Study, UK public-health guidance, and mechanistic plausibility. [1–13]
The most important shift is away from the old assumption that only high-level lead poisoning matters. Public-health guidance now recognises that there is no safe threshold for lead exposure in children, and England’s public-health intervention concentration for children and pregnant women has been lowered from 10 µg/dL to 5 µg/dL. Even that action point is not a safety line. It is a trigger for investigation, monitoring and source control. [2–5]
For older homes, especially homes with babies, young children or pregnant women, this has direct practical consequences. Bottle-fed infants may be exposed repeatedly if formula is made up with tap water that has stood in contact with lead pipework, solder or fittings. That does not make formula feeding the problem. It makes legacy plumbing the problem. [1,14–16]
The public-health answer is therefore not complacency, and not panic. It is source identification and removal. In older housing, that means considering lead paint, contaminated dust and soil, imported products, and historic plumbing. Where lead pipework is present, replacement is not merely a property upgrade. It is a neurodevelopmental prevention measure. [1,2,13,15–17]
Disclosure
This article is published by London & Surrey Water Services Ltd, a CIPHE member and WaterSafe approved contractor whose business includes lead pipe replacement. The company therefore has a commercial interest in the subject matter. The article is restricted to findings and positions reported in the sources cited, and no claim is made here that is not traceable to those sources. It is not medical advice. Readers concerned about lead exposure should speak to their GP, and readers concerned about lead in their own water supply should contact their water supplier or seek independent laboratory testing.
References
- World Health Organization. Childhood lead poisoning. Geneva: World Health Organization; 2010.
- Public Health England. Evaluation of whether to lower the public health intervention concentration for lead exposure in children. London: Public Health England; 2021.
- UK Health Security Agency. Lead: environmental and public health intervention. London: UKHSA; updated guidance.
- UK Health Security Agency. Lead: clinical intervention. London: UKHSA; updated guidance.
- World Health Organization. Lead poisoning and health. Geneva: World Health Organization; 2024.
- Rosenauer V, Schwarz MI, Vlasak T, Barth A. Childhood lead exposure increases the risk of attention-deficit-hyperactivity disorder: a meta-analysis. Science of the Total Environment. 2024;951:175574.
- Dalla MBD, Ayala CO, Castro FCAQ, Neto FK, Zanirati G, Cañon-Montañez W, et al. Environmental pollution and attention deficit hyperactivity disorder: a meta-analysis of cohort studies. Environmental Pollution. 2022;315:120351.
- Ji Y, Hong X, Wang G, Chatterjee N, Riley AW, Lee LC, et al. A prospective birth cohort study on early childhood lead levels and attention deficit hyperactivity disorder: new insight on sex differences. Journal of Pediatrics. 2018;199:124–131.e8.
- Huang S, Hu H, Sánchez BN, Peterson KE, Ettinger AS, Lamadrid-Figueroa H, et al. Childhood blood lead levels and symptoms of attention deficit hyperactivity disorder (ADHD): a cross-sectional study of Mexican children. Environmental Health Perspectives. 2016;124(6):868–874.
- Thomson GO, Raab GM, Hepburn WS, Hunter R, Fulton M, Laxen DP. Blood-lead levels and children’s behaviour: results from the Edinburgh Lead Study. Journal of Child Psychology and Psychiatry. 1989;30(4):515–528.
- Nigg JT, Knottnerus GM, Martel MM, Nikolas M, Cavanagh K, Karmaus W, et al. Low blood lead levels associated with clinically diagnosed attention-deficit/hyperactivity disorder and mediated by weak cognitive control. Biological Psychiatry. 2008;63(3):325–331.
- Lanphear BP, Hornung R, Khoury J, Yolton K, Baghurst P, Bellinger DC, et al. Low-level environmental lead exposure and children’s intellectual function: an international pooled analysis. Environmental Health Perspectives. 2005;113(7):894–899.
- Crabbe H, Verlander NQ, Iqbal N, Close R, White G, Leonardi GS, Busby A. ‘As safe as houses’; the risk of childhood lead exposure from housing in England and implications for public health. BMC Public Health. 2022;22:2052.
- NHS. How to make up a feed. Best Start in Life. NHS website.
- Drinking Water Inspectorate. Lead in drinking water. DWI website.
- Thames Water. Lead and Lead pipe replacement scheme. Customer guidance pages, Thames Water website.
- Thames Water. TMS22 Enhancement Case: Long Term Water Quality Strategy Lead. Thames Water regulatory publication.
