Abstract
Lead contamination of drinking water from legacy plumbing remains a significant public-health concern globally. Although the use of lead in new drinking-water pipework has been prohibited or heavily restricted in many high-income countries for decades, older lead service lines, communication pipes, customer-side supply pipes, leaded solder, brass fittings and internal plumbing can still release lead into tap water. The United Kingdom developed one of the most extensive water-industry programmes of plumbosolvency control during the late twentieth century, particularly in regions supplied by soft, low-alkalinity waters.
Following national surveys and epidemiological studies in the 1970s and early 1980s, UK water authorities adopted a staged corrosion-control strategy. Initial interventions focused on pH correction, commonly through lime dosing, followed by widespread orthophosphate dosing from the late 1980s and 1990s onwards. This article traces the evolution of the UK approach, examines the scientific mechanism of orthophosphate treatment, and reviews evidence for its effectiveness in reducing both tap-water lead and blood lead concentrations.
The UK experience is then compared with approaches in the United States, Canada, the Netherlands, Germany, Australia and New Zealand. The comparison shows that corrosion-control treatment can deliver substantial and rapid public-health benefits, but it does not remove the underlying source of exposure. As regulatory standards tighten and expectations move toward lower lead concentrations at the consumer tap, the policy centre of gravity is shifting from chemical suppression of plumbosolvency toward progressive removal of lead-bearing pipework and fittings. The UK case therefore offers two lessons for international practice: corrosion control can be highly effective as an interim protective measure, but long-term lead-risk reduction ultimately depends on removing lead-bearing materials from drinking-water systems.
Table of Contents
Introduction
Lead remains one of the most significant chemical contaminants in drinking water worldwide. In most modern drinking-water systems, lead is not normally present in treated water leaving water treatment works. Instead, it enters drinking water after treatment through contact with legacy lead pipes, leaded solder, brass fittings and other lead-bearing plumbing materials. This is particularly important in older housing stock, where original service lines, communication pipes, customer-side supply pipes or internal pipework may still be present.
The dissolution of lead from pipework and plumbing materials is known as plumbosolvency. It is strongly influenced by water chemistry. Waters that are soft, acidic and low in alkalinity are especially aggressive toward lead because they lack the buffering capacity and mineral content required to form stable protective scales on pipe surfaces (Schock, 1980; Schock, Wagner and Oliphant, 1996). Under such conditions, lead can dissolve into drinking water even where the wider distribution system is otherwise well controlled.
The health basis for controlling lead exposure is now clear. There is broad scientific consensus that no level of lead exposure is known to be entirely safe. Children, infants and unborn babies are particularly vulnerable because lead can impair neurodevelopment, behaviour and cognitive outcomes. Maternal exposure during pregnancy can also affect fetal development. These risks have driven progressive tightening of drinking-water standards and increasing regulatory pressure to reduce lead at the consumer tap.
The United Kingdom has one of the longest and most systematically documented experiences of managing plumbosolvency at scale. The UK response developed through a combination of regional water-authority action, water-company treatment optimisation, national regulation and public-health research. It began with recognition of a widespread problem in the 1970s, particularly in Scotland and other areas supplied by soft upland waters. It then developed into a staged programme of pH correction followed by orthophosphate dosing.
The central argument of this article is that the UK experience demonstrates both the power and the limits of corrosion-control treatment. pH correction and orthophosphate dosing can substantially reduce lead release and deliver rapid population-level benefits, particularly where legacy lead pipework cannot be removed quickly. However, these measures do not remove the source of exposure. As standards tighten and as regulators move toward lower lead limits, long-term strategy increasingly requires the progressive removal of lead-bearing pipework and fittings.
This article first reviews the historical development of plumbosolvency control in the UK. It then explains the mechanism of orthophosphate treatment and evaluates evidence of effectiveness. It then compares the UK experience with international approaches in the United States, Canada, the Netherlands, Germany, Australia and New Zealand, distinguishing between corrosion-control-led, replacement-led and product-control-led regulatory models. The final sections consider the limitations of orthophosphate dosing and identify lessons for future drinking-water policy.
Recognition of the Problem in the UK
Lead pipes had been used in water supply systems for centuries, but the full scale of lead contamination from drinking water became widely recognised in the United Kingdom during the 1970s. Before this period, elevated lead levels were often treated as localised technical problems rather than as a broader public-health issue.
The turning point came through national surveys and government-commissioned expert reviews that revealed elevated lead concentrations in a significant proportion of household tap-water samples. The problem was especially marked in areas supplied by soft, acidic upland waters. Scotland became one of the clearest case studies. Glasgow, supplied by the soft Loch Katrine source, showed particularly high levels of water lead. A 1977 survey found that 83% of sampled households exceeded 50 µg/L, with many homes recording concentrations above 100 µg/L (Richards and Moore, 1984; Watt et al., 2000).
The severity of the Scottish problem reflected the interaction of three factors: extensive use of lead pipework, aggressive soft water, and limited natural formation of protective pipe scales. Soft waters with low alkalinity and low pH are more likely to dissolve lead because they do not readily form stable carbonate or phosphate scales on pipe surfaces (Moore, 1985).
Epidemiological studies in Glasgow and Ayr during the late 1970s and early 1980s demonstrated associations between elevated water lead and increased blood lead concentrations, including among mothers and young children (Sherlock et al., 1982; Sherlock et al., 1984). Bottle-fed infants were identified as a particularly vulnerable group because infant formula prepared with contaminated tap water could substantially increase lead intake.
These findings created strong pressure for corrective treatment. The first large-scale response was pH adjustment.
Initial Response: pH Correction
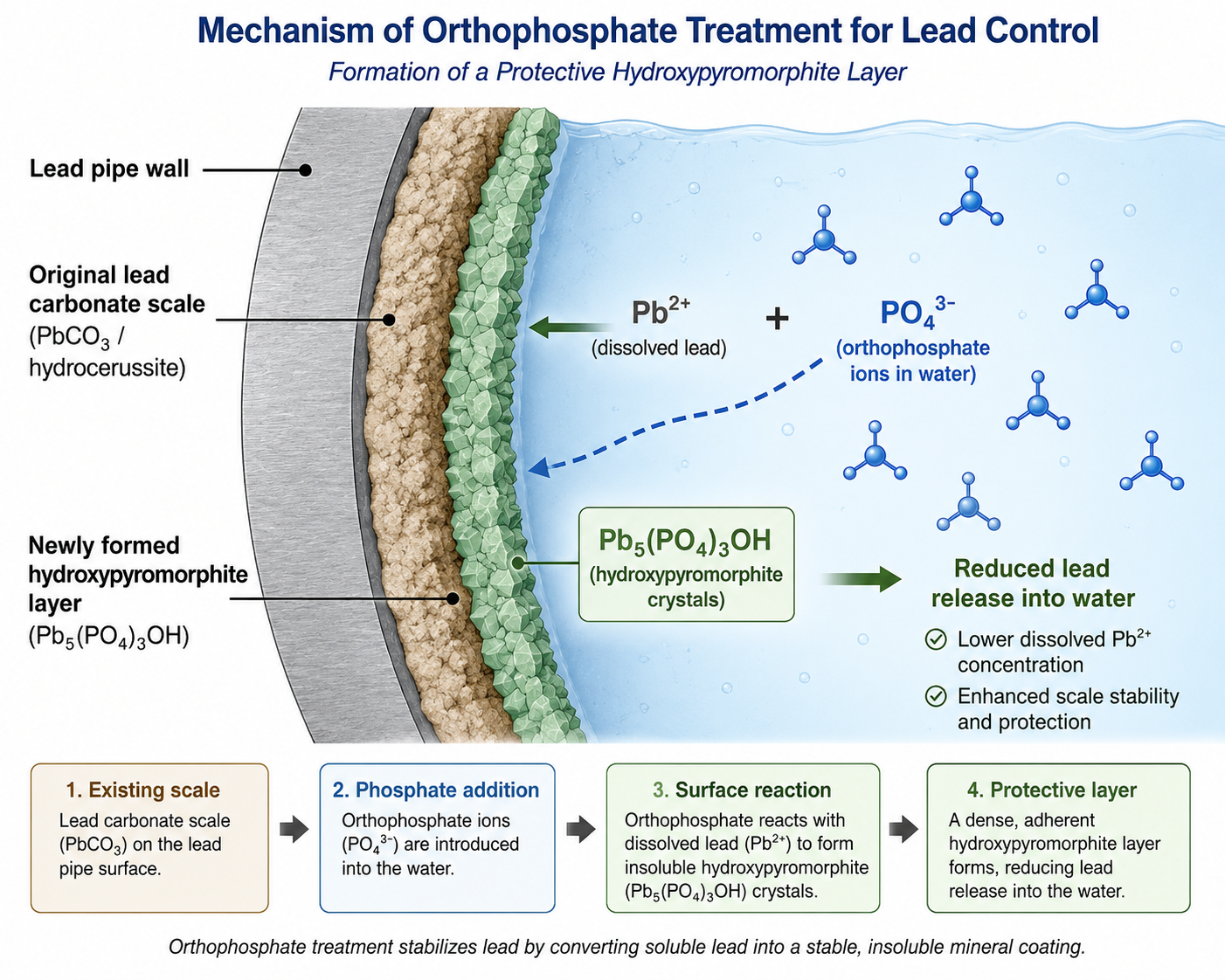
The first major corrosion-control intervention in the UK was pH correction, primarily through lime dosing. Raising pH reduces plumbosolvency by encouraging the formation of less soluble lead carbonate scales on pipe surfaces. These scales act as a partial barrier between the water and the underlying lead pipe (Schock, 1980).
Automatic lime-dosing systems began operating in Glasgow and Edinburgh in 1978. On the Loch Katrine supply serving Glasgow, pH was raised from approximately 6.3 to around 7.8 (Moore, 1985; Higney, Hanley and Moro, 2025). Ayr’s more acidic supply was treated shortly afterwards, with treatment to reduce plumbosolvency initiated in 1981 (Sherlock et al., 1984).
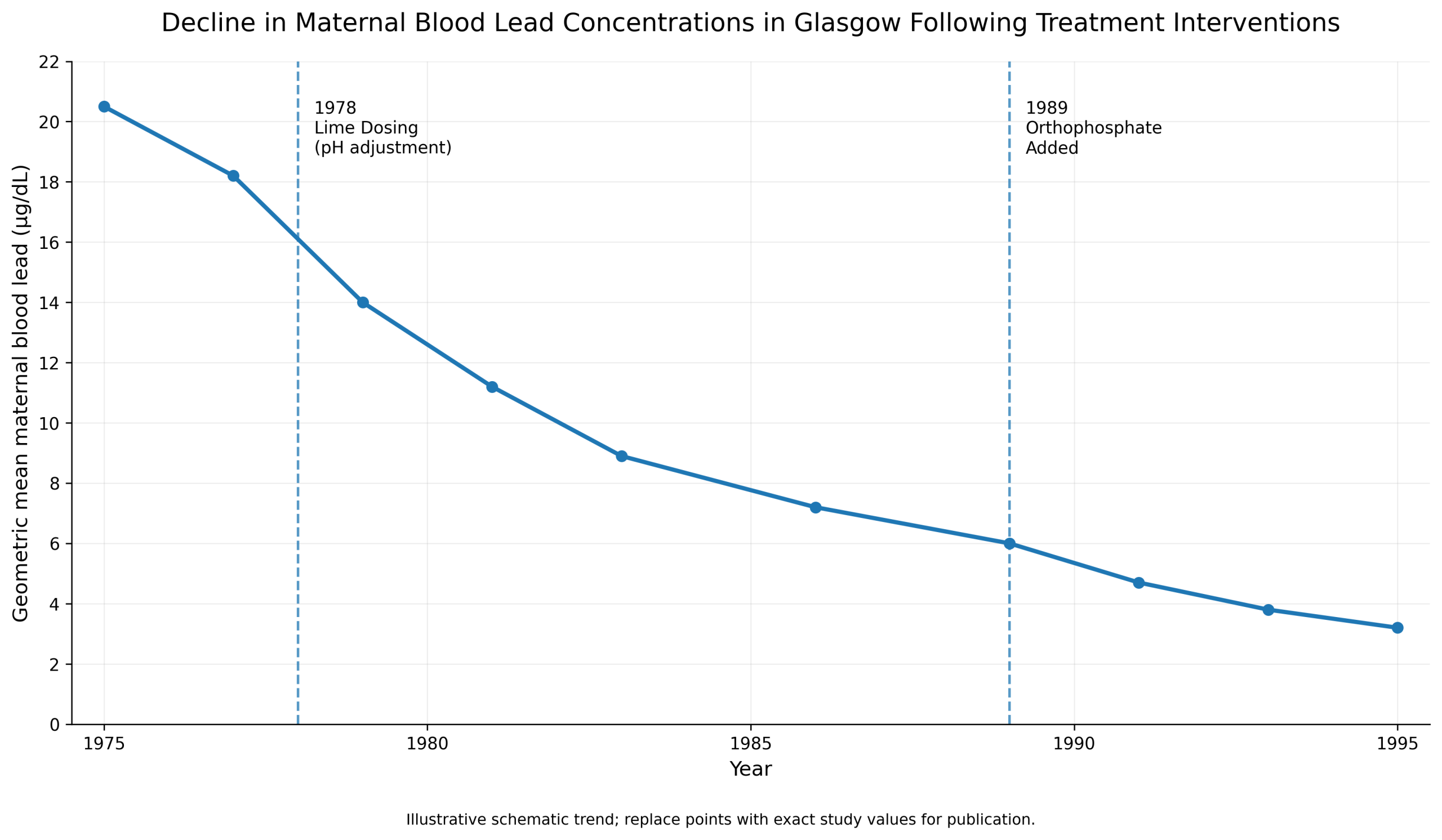
The early results were encouraging. In Ayr, treatment was associated with a fall in median blood lead among sampled women from 21 to 13 µg/100 ml (Sherlock et al., 1984). In Glasgow, lime dosing produced a substantial fall in maternal blood lead by 1980. These changes demonstrated that water treatment could produce measurable public-health benefits.
However, pH correction had limitations. In very soft waters, residual plumbosolvency could remain significant even after pH adjustment. Protective carbonate scales could be incomplete, unstable or slow to develop. In some areas, compliance with increasingly stringent lead standards required additional treatment. These limitations led to the adoption of orthophosphate dosing.
Orthophosphate Treatment: Introduction and Mechanism
By the late 1970s and early 1980s, UK water engineers and public-health researchers recognised that pH correction alone would not always provide sufficient control. Orthophosphate dosing emerged as a complementary treatment, especially where soft waters continued to release lead after pH adjustment.
Early technical assessments of pH correction and orthophosphate addition appeared in UK water-engineering literature in the early 1980s (Sheiham and Jackson, 1981). Operational work on plumbosolvency control in hard waters followed later in the decade (Colling, Whincup and Hayes, 1987; Colling et al., 1992). In Scotland, orthophosphate was added to the Glasgow supply in 1989 (Watt et al., 2000).
Evidence of Effectiveness in the UK
The evidence for the UK’s staged corrosion-control approach comes from operational monitoring, public-health studies and long-term compliance data.
Glasgow provides one of the clearest examples. The combination of lime dosing from 1978 and orthophosphate addition from 1989 was associated with substantial reductions in tap-water lead. Watt et al. (1996) reported that the proportion of households with water lead at or above 10 µg/L fell from 49% in 1981 to 17% in 1993. However, tap-water lead remained the main correlate of raised maternal blood lead concentrations, showing both the effectiveness and incompleteness of treatment.
The Ayr studies provide strong before-and-after evidence. Sherlock et al. (1984) found that treatment of the Ayr supply was associated with a reduction in median women’s blood lead from 21 to 13 µg/100 ml. This was important because it showed that treating plumbosolvent water could reduce internal human exposure, not merely improve water-sample results.
Later UK experience focused on optimising orthophosphate doses by water supply zone. Laboratory plumbosolvency testing, zonal modelling and operational monitoring allowed water companies to adjust treatment to local water chemistry. Cardew (2009), Hayes, Incledion and Balch (2008), and Hayes and Hydes (2012) all contributed to the evidence base showing that orthophosphate dosing could substantially improve compliance with the 10 µg/L standard.
In England and Wales, the prescribed concentration or value for lead at the consumer tap is 10 µg/L under the Water Supply (Water Quality) Regulations. A 2021 WRc report commissioned by the DWI modelled the costs and benefits of moving to a 5 µg/L standard, evaluating both a 10-year and a 15-year remediation programme in high-risk supply zones, targeting compliance by 2035 or 2040 respectively, with further remediation toward no detectable lead modelled out to 2055–2070 (Hulance, Kowalski and Fairhurst, 2021). A Water Advisory Group convened by the DWI subsequently recommended in December 2024 that the standard be formally tightened to 5 µg/L, alongside a national lead-removal strategy, though as of that report neither recommendation had yet been enacted in law (Drinking Water Inspectorate, 2024a).
Nevertheless, residual risks remain. Some properties with long lead supply pipes, internal lead plumbing, leaded solder or disturbed corrosion scales can still exceed standards. Compliance sampling may also under-detect episodic release, especially where lead particles are mobilised after disturbance. Modern UK strategy therefore increasingly combines continued corrosion-control treatment with progressive pipe replacement.
Thames Water’s own investment case makes this transition explicit. It states that lead in drinking water comes from lead pipes, not treatment works; that responsibility is split between the water company’s communication pipe and the customer’s private supply pipe, with the company responsible only up to the outside stop valve; and that communication-pipe replacement alone does not fully remove the public-health and compliance risk where customer-side lead remains (Thames Water, 2024).
International Regulatory and Strategic Comparison
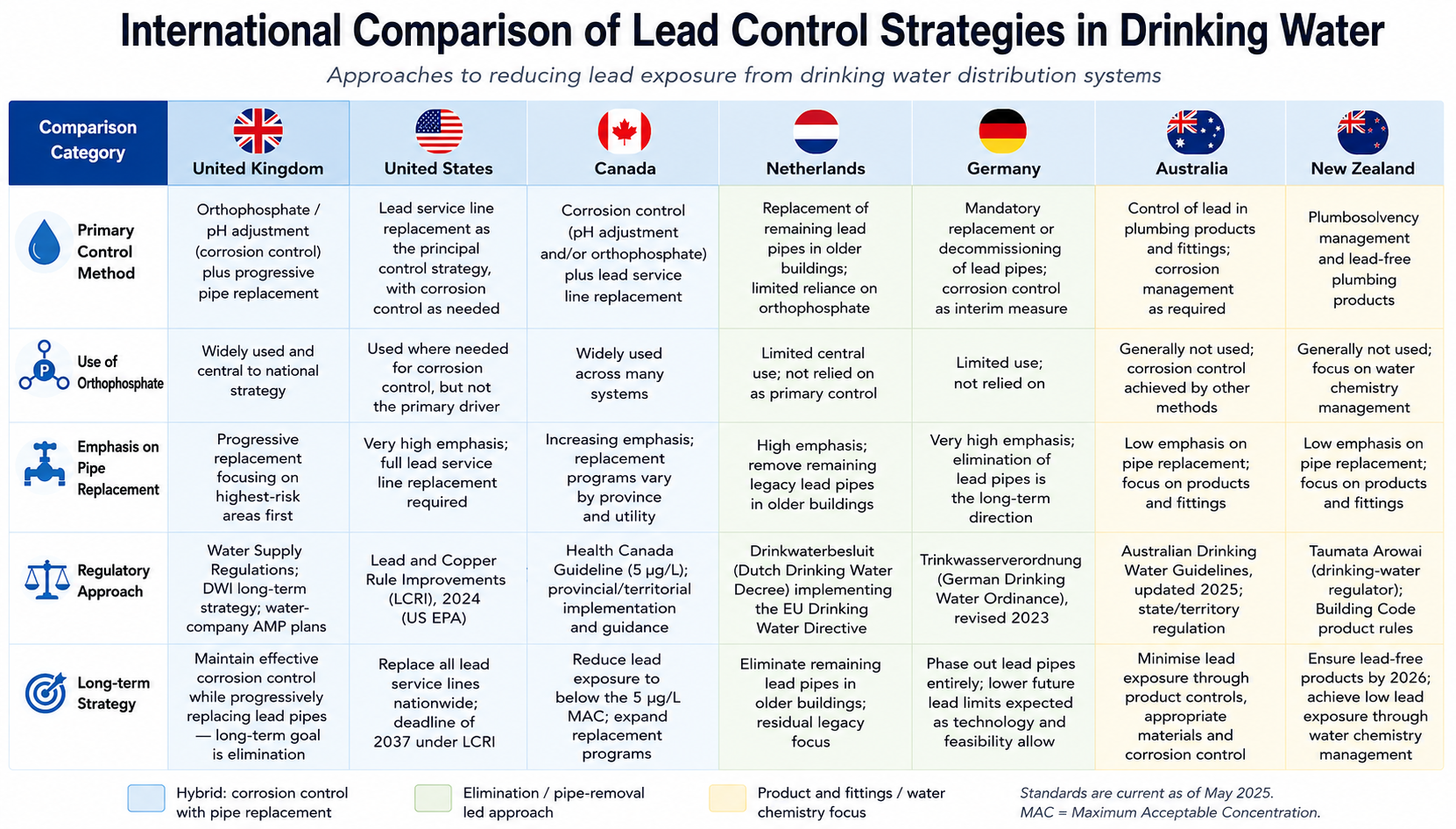
International experience shows three broad models of lead control.
The first is the hybrid corrosion-control and replacement model, seen most clearly in the United States, Canada and the United Kingdom. These systems rely on corrosion-control treatment while lead service lines or lead-bearing private supply pipes remain in place, but are increasingly moving toward mandatory or accelerated replacement.
The second is the elimination-led model, seen most clearly in Germany and, to a lesser extent, the Netherlands. In this model, the policy emphasis has shifted toward removing or prohibiting remaining lead pipework rather than relying indefinitely on water-treatment chemistry.
The third is the plumbing-product and water-chemistry model, seen in Australia and New Zealand. Here, the issue is less a nationally dominant buried lead-service-line stock and more a combination of corrosive water, plumbing products, fittings and residual older building materials.
United States
The United States historically relied on corrosion control as the central regulatory tool for managing lead in drinking water. The Lead and Copper Rule, introduced in 1991 under the Safe Drinking Water Act, established an action-level framework rather than a conventional maximum contaminant level. Utilities were required to monitor lead at high-risk taps and implement corrosion control where action levels were exceeded.
Two major crises exposed the fragility of this approach. In Washington, D.C., a change to chloramine disinfection in the early 2000s destabilised existing scales and increased lead release from service lines. In Flint, Michigan, the 2014 switch in source water without legally required corrosion control produced a major public-health failure and became an international example of how treatment changes can destabilise lead control.
In response, the United States has moved toward a replacement-led hybrid model. EPA’s 2024 Lead and Copper Rule Improvements require drinking-water systems to identify and replace lead pipes within 10 years, strengthen testing requirements and lower the threshold requiring action to protect consumers (US EPA, 2024a; 2024b). The rule therefore marks a major shift: corrosion control remains necessary while lead service lines remain in place, but full replacement has become the central long-term compliance strategy.
The United States differs from the UK in scale and ownership complexity. Lead service lines remain a major buried-network problem across many cities. Estimates of the remaining national stock are disputed even within EPA’s own publications: a 2023 Drinking Water Infrastructure Needs Survey put the figure at 9.2 million lines nationally, while more recent EPA statements cite roughly 4 million — illustrating how uncertain even official federal inventories remain (US EPA, 2023; 2019). Full replacement also requires coordination between public-side and private-side pipe ownership. These challenges closely resemble the UK’s unresolved customer-side supply pipe problem, but at a much larger national scale.
Canada
Canada occupies a similar hybrid position, but with more decentralised implementation. Health Canada’s 2019 guideline set a maximum acceptable concentration of 5 µg/L for lead in drinking water, measured at the tap (Health Canada, 2019). However, drinking-water regulation is implemented primarily by provinces and territories, so practical approaches vary.
Health Canada’s guidance explicitly supports both corrosion control and full lead service line replacement. It recognises that lead service lines can be a major contributor to tap-water lead after stagnation and that partial replacement can increase short-term exposure by disturbing existing scales. The preferred long-term strategy is full removal, but corrosion control remains important while lead-bearing materials remain in place.
Toronto illustrates the Canadian hybrid model. The city introduced orthophosphate dosing in 2014 as part of its Lead in Drinking Water Mitigation Strategy while continuing public-side lead service replacement. Its 2025 annual lead mitigation reporting still recorded an estimated 13,664 public-side lead service lines remaining (City of Toronto, 2026; 2011), showing that treatment and replacement continue to operate together rather than sequentially.
Canada therefore demonstrates the same central lesson as the UK: corrosion control reduces exposure but does not remove the source. Where service lines remain, the long-term policy question becomes how to fund, compel and coordinate full replacement across public and private ownership boundaries.
Netherlands
The Netherlands has moved closer to an elimination model. Lead drinking-water pipes were prohibited in new installations from 1960, and utility-side lead pipes have largely been replaced up to the property boundary (RIVM, 2025). Remaining risks are concentrated mainly in older buildings, particularly pre-1960 homes, apartments and institutional buildings where internal lead pipework may still exist. An estimated 200,000 Dutch dwellings still had lead pipes as of 2020–2021 (RIVM, 2019).
Dutch public-health attention has focused on identifying and replacing remaining lead pipes inside buildings, with particular concern for infants, young children and pregnant women. The Netherlands therefore differs from the United States and Canada because the main policy challenge is no longer a large national stock of buried lead service lines. Instead, the issue is residual building-level plumbing.
This makes the Dutch model more housing-policy oriented than treatment-policy oriented. Water chemistry still matters, but the dominant long-term approach is identifying older buildings, informing owners and replacing remaining internal lead pipework.
Germany
Germany offers the strongest elimination-led comparison. The amended Drinking Water Ordinance, effective from June 2023, prohibits lead pipes and requires remaining lead pipes and lead pipe parts to be removed by 12 January 2026. Germany’s Federal Environment Agency states that the 10 µg/L limit cannot usually be met where drinking water flows through lead pipes (Umweltbundesamt, 2023).
This is a fundamentally different regulatory posture from systems that rely on corrosion control to manage lead release. Germany’s position treats lead pipes themselves as incompatible with long-term compliance. The pipe material must be removed or decommissioned, rather than merely controlled chemically.
Germany’s residual lead-pipe stock is now comparatively small — around 15,000 lead house-connection lines and 38,000 buildings with lead internal plumbing, at a total remediation cost of up to €100 million (Umweltbundesamt, 2023). This reflects earlier restrictions, replacement activity and a regulatory culture that places strong emphasis on material suitability. As a result, Germany did not need to develop a national orthophosphate programme comparable to the UK’s. The German example shows what policy can look like once the residual lead-pipe stock becomes small enough for mandatory elimination to be practical.
Australia
Australia represents a different pattern. The national issue is not generally framed around a large buried stock of lead service lines comparable to North America. Instead, concern has focused on lead leaching from plumbing products, brass fittings, taps, solders and other materials in contact with drinking water.
The Australian Drinking Water Guidelines were updated in 2025. The National Health and Medical Research Council now states that, based on health considerations, lead in drinking water should not exceed 0.005 mg/L, equivalent to 5 µg/L (NHMRC, 2025).
Australia therefore combines stricter health-based guidance with a product-control and corrosion-management focus. pH and alkalinity adjustment, and in some settings phosphate-based corrosion control, remain relevant tools. However, unlike the United States, Australia has not developed a national lead service line replacement programme as the central policy response.
New Zealand
New Zealand’s approach centres on plumbosolvency, naturally aggressive water and plumbing-product control. Taumata Arowai has emphasised that some New Zealand drinking waters can dissolve metals from plumbing materials, making water chemistry and consumer advice important parts of risk management (Taumata Arowai, 2025).
New Zealand has also moved toward tighter product controls. From 2 May 2026, drinking-water plumbing products used in new building consents must be lead-free (Taumata Arowai, 2026). This aligns New Zealand with a broader international shift away from managing lead release after installation and toward preventing lead-bearing materials from entering drinking-water systems in the first place.
New Zealand’s most prominent recent lead incident, affecting Waikouaiti, Karitane and Hawksbury Village in 2021, was not a simple analogue of Flint or Washington, D.C. It was linked to lead-containing materials in water-supply assets rather than a national buried lead service line issue (Dunedin City Council, 2021). The New Zealand case therefore reinforces a different lesson: in countries without a major lead service line stock, product standards, asset materials and plumbosolvency management may be the key control points
Positioning the UK Internationally
Set against these comparators, the UK sits closest to the hybrid model. Like the United States and Canada, it relies on corrosion-control treatment while lead-bearing materials remain in place. Like Germany and the Netherlands, it increasingly recognises that long-term risk reduction requires removal. The difference is that the UK still has a substantial unresolved stock of lead communication pipes, customer-side supply pipes and internal plumbing, and the responsibility boundary between water company and property owner complicates delivery.
Thames Water’s lead strategy illustrates this tension clearly. It identifies lead pipework in contact with drinking water as an immediate public-health risk, proposes 54,000 lead communication-pipe replacements in AMP8, and recognises that customer-side supply pipes remain a major unresolved part of the problem. It also states that at the current replacement rate, removing all Thames Water lead communication pipes would take until 2135, well beyond the Drinking Water Inspectorate’s 2050 ambition for a lead-free network (Thames Water, 2024; Drinking Water Inspectorate, 2024b).
This makes the UK a useful international case study. It shows that chemical corrosion control can protect public health over decades, but it also shows how difficult it is to move from exposure reduction to source elimination when ownership, cost and access are split between utilities and private property owners.
Limitations, Trade-Offs and Ongoing Challenges
The UK’s corrosion-control approach has delivered substantial public-health benefits, but it has important limitations.
The first limitation is that treatment does not remove the source. Orthophosphate dosing can reduce lead release, but lead-bearing pipework remains in contact with drinking water. Disturbance, stagnation, hydraulic changes, local water-chemistry shifts or partial pipe replacement can still mobilise lead.
The second limitation is that treatment takes time to stabilise. Orthophosphate is not an instant barrier. Lead phosphate phases must form and become sufficiently stable to control release (Colling, Croll, Whincup and Harward, 1992). During this period, some properties may continue to experience elevated concentrations.
The third limitation is variability. Orthophosphate performance depends on water chemistry, pipe condition, dose, pH, alkalinity, stagnation time and the nature of existing corrosion scales. Very soft waters, high organic matter or disturbed pipe scales can produce less predictable outcomes.
The fourth limitation is environmental. Orthophosphate dosing increases phosphorus loads entering wastewater systems, with one estimate placing it at around 5% of the total phosphorus load in UK domestic wastewater, although contributions vary by catchment and treatment configuration (Comber et al., 2013, cited in POST, 2014). While the contribution from drinking-water treatment is only one part of the broader phosphorus pollution, it remains relevant in catchments already under eutrophication pressure.
The fifth limitation is resource dependence. Orthophosphate used in water treatment is derived from phosphate rock, a finite mineral resource concentrated in a small number of countries — primarily North Africa (64% of known reserves), the USA (15%), and China (6%) — which has led the EU to add phosphate rock to its list of critical raw materials (POST, 2014). This dependence has direct practical consequences: the efficacy of orthophosphate dosing diminishes with increasing dose, such that it is extremely unlikely water companies could ever achieve full compliance with the current, or any future lower, water quality standard through conditioning alone (Hulance, Kowalski and Fairhurst, 2021). Thames Water’s own strategy separately notes that orthophosphoric acid is already a significant operational cost (Thames Water, 2024). These factors make indefinite expansion of phosphate dosing unattractive as a long-term policy endpoint.
A final limitation is regulatory trajectory. The lower the lead standard becomes, the harder it is for chemical treatment alone to guarantee compliance at every consumer tap. Thames Water’s own assessment states that its current orthophosphoric acid mitigation is reaching the limit of the protection it can offer, and that any tightening of the 10 µg/L standard will challenge the company’s ability to achieve compliance through treatment alone (Thames Water, 2024).
Taken together, these limitations do not undermine the value of orthophosphate. They clarify its proper role. Orthophosphate is a highly effective protective measure while lead remains in the system. It is not a substitute for removing lead-bearing materials
Implications for UK Lead Policy
The UK now faces a strategic transition. The historical success of pH correction and orthophosphate dosing has reduced exposure and improved compliance. However, future progress depends on moving from plumbosolvency control to lead removal.
This transition has several practical implications.
First, water companies must maintain corrosion control while lead pipework remains in contact with drinking water. Premature withdrawal of orthophosphate could increase exposure.
Second, replacement programmes need to consider the full source-to-tap system: communication pipe, customer-side supply pipe, internal stop valve, internal plumbing and kitchen tap. Replacing only the water-company section may reduce risk but can leave significant residual exposure where private lead pipework remains.
Third, lead-risk targeting should use careful evidence. Housing age is a useful proxy because older properties are more likely to contain legacy pipe materials, but it is not proof that a specific property has lead pipework. Prioritisation models based on housing age and other risk indicators can support targeting, but confirmation always requires inspection, testing or pipe-material verification. This distinction matters for both public communication and operational planning.
Fourth, customer-side replacement remains the central unresolved challenge, complicated by the fact that property owners are often reluctant to replace their portion of the pipe and that the exact location of most remaining lead service pipes is not well recorded (Hulance, Kowalski and Fairhurst, 2021). Thames Water’s AMP8 plan includes a customer trial to explore education, financial support and delivery options for removing customer-side lead supply pipes (Thames Water, 2024). This is critical because long-term compliance at the consumer tap cannot be guaranteed if private pipework remains outside replacement programmes.
Finally, public messaging must be accurate. The correct message is not that every older home has lead pipes. It is that older properties are more likely to contain legacy pipe materials and should be checked where lead risk is plausible.
Lessons for International Practice
The UK experience offers several lessons for countries still managing lead in drinking water.
Corrosion control can deliver rapid public-health gains. The UK evidence from Glasgow, Ayr and later water-company optimisation shows that pH correction and orthophosphate dosing can substantially reduce tap-water lead and blood lead concentrations. For countries with extensive legacy pipework, corrosion control remains essential while replacement programmes are planned and delivered.
Treatment must be optimised locally. There is no universal orthophosphate dose that works equally across all systems. Treatment must be adapted to pH, alkalinity, water source, pipe condition, stagnation patterns and existing scales. Poorly managed treatment transitions can destabilise corrosion control, as shown by major US incidents.
Pipe replacement is the only permanent source-control measure — and can be economically justified. Germany and the Netherlands show the direction of travel once residual lead-pipe stocks become manageable: legal and housing-policy tools can displace indefinite reliance on corrosion-control chemistry. The United States and Canada are now also moving toward replacement-led strategies, although at much greater scale and cost. The UK’s own economic modelling supports this direction: the DWI’s commissioned cost-benefit analysis found that replacing lead service pipes to the consumer’s compliance tap is highly likely to be cost-beneficial in high-risk supply zones, and likely cost-beneficial in medium- and low-risk zones, when implemented over a 10–15-year period (Hulance, Kowalski and Fairhurst, 2021).
Ownership boundaries are a central barrier. Lead pipework often crosses responsibility boundaries. In the UK, water companies are responsible for communication pipes, while property owners are responsible for private supply pipes and internal plumbing. Similar public/private ownership issues occur in North America. Without a mechanism for customer-side replacement, full lead-risk removal remains incomplete.
Product standards matter. Australia and New Zealand show that even where lead service lines are not the dominant issue, lead can still enter drinking water through plumbing products, fittings and materials. Lead-free product standards are therefore an essential part of prevention.
Chemical control should be treated as interim protection, not the endpoint. Orthophosphate is highly effective, but it depends on continuous dosing, stable water chemistry, careful monitoring and a finite resource. It reduces exposure; it does not eliminate the source. Long-term drinking-water policy should therefore combine corrosion control with planned removal of lead-bearing materials.
Conclusion
The UK developed one of the most extensive and influential water-industry approaches to plumbosolvency control. Beginning with recognition of severe lead contamination in soft-water areas during the 1970s, the UK moved through pH correction, lime dosing and then widespread orthophosphate treatment. These interventions produced substantial reductions in tap-water lead and blood lead concentrations and remain an important public-health success.
However, the UK experience also demonstrates the limits of chemical control. Orthophosphate works by suppressing lead release; it does not remove lead-bearing pipework. It requires time to stabilise, performs variably across water chemistries, adds phosphorus to wastewater, depends on a finite phosphate resource and becomes less reliable as standards move lower.
International comparison reinforces this conclusion. The United States and Canada show the risks of long-term reliance on corrosion control where lead service lines remain widespread. Germany and the Netherlands show a more elimination-led future, where remaining lead pipes are treated as materials to be removed rather than controlled chemically. Australia and New Zealand show the importance of plumbing-product standards and water-chemistry management where lead service lines are not the dominant national problem.
The central lesson is therefore clear. Corrosion-control treatment is a vital protective measure, especially where immediate full replacement is impractical. But the sustainable long-term objective is not better management of lead pipes. It is the progressive removal of lead-bearing materials from the drinking-water pathway, from utility pipework through to the consumer tap.
References
Cardew, P.T. (2009) ‘Measuring the benefit of orthophosphate treatment on lead in drinking water’, Journal of Water and Health, 7(1), pp. 123–131.
City of Toronto (2011) Lead in Drinking Water Mitigation Strategy. Toronto: City of Toronto.
City of Toronto (2026) 2025 Annual Report – Lead in Drinking Water Mitigation Strategy. Toronto: City of Toronto.
Colling, J.H., Croll, B.T., Whincup, P.A.E. and Harward, C. (1992) ‘Plumbosolvency effects and control in hard waters’, Water and Environment Journal, 6(3), pp. 259–268.
Colling, J.H., Whincup, P.A.E. and Hayes, C.R. (1987) ‘The measurement of plumbosolvency propensity to guide the control of lead in tap waters’, Water and Environment Journal, 1(3), pp. 263–269.
Drinking Water Inspectorate (2024a) Drinking Water Quality Standards in England and Wales: Recommendations and Full Report of the Advisory Group, December 2024.
Drinking Water Inspectorate (2024b) Thames Water Utilities Limited – AMP8 Lead Strategy. Available at: https://www.dwi.gov.uk/water-companies/improvement-programmes/thames-water-improvement-programmes/tms-2023-00013-v1/
Dunedin City Council (2021) Waikouaiti Metals – Investigation Report. Dunedin: Dunedin City Council.
Hayes, C.R., Incledion, S. and Balch, M. (2008) ‘Experience in Wales (UK) of the optimisation of ortho-phosphate dosing for controlling lead in drinking water’, Journal of Water and Health, 6(2), pp. 177–190.
Hayes, C.R. and Hydes, O.D. (2012) ‘UK experience in the monitoring and control of lead in drinking water’, Journal of Water and Health, 10(3), pp. 337–348.
Health Canada (2019) Guidelines for Canadian Drinking Water Quality: Guideline Technical Document – Lead. Ottawa: Government of Canada.
Higney, A., Hanley, N. and Moro, M. (2025) ‘The impact of lead water pollution on birth outcomes: A natural experiment in Scotland’, Environmental and Resource Economics, 88, pp. 3737–3764.
Hulance, J., Kowalski, M. and Fairhurst, R. (2021) Long-term Strategies to Reduce Lead Exposure from Drinking Water. Report Reference DWI14372.2. Swindon: WRc, for the Drinking Water Inspectorate.
Moore, M.R. (1985) ‘Influence of acid rain upon water plumbosolvency’, Environmental Health Perspectives, 63, pp. 121–126.
National Health and Medical Research Council (2025) Australian Drinking Water Guidelines: Lead. Canberra: NHMRC.
Parliamentary Office of Science and Technology (POST) (2014) Phosphate Resources. POSTnote 477. London: Houses of Parliament.
Richards, W.N. and Moore, M.R. (1984) ‘Lead hazard controlled in Scottish water systems’, Journal AWWA, 76(8), pp. 60–67.
RIVM (2019) Lead exposure via tap water at times too high. Bilthoven: National Institute for Public Health and the Environment.
RIVM (2025) Loden leidingen – Drinkwater. Bilthoven: National Institute for Public Health and the Environment.
Schock, M.R. (1980) ‘Response of lead solubility to dissolved carbonate in drinking water’, Journal AWWA, 72(12), pp. 695–704.
Schock, M.R. and Clement, J.A. (1998) ‘Lead and copper control with non-zinc orthophosphate’, Journal of the New England Water Works Association, 112(2), pp. 20–42.
Schock, M.R., Wagner, I. and Oliphant, R.J. (1996) ‘The corrosion and solubility of lead in drinking water’, in Internal Corrosion of Water Distribution Systems. 2nd edn. Denver, CO: AWWA Research Foundation.
Sheiham, I. and Jackson, P.J. (1981) ‘The scientific basis for control of lead in drinking water by water treatment’, Journal of the Institution of Water Engineers and Scientists, 35(6), pp. 491–515.
Sherlock, J.C., Ashby, D., Delves, H.T., Forbes, G.I., Moore, M.R., Patterson, W.J., Pocock, S.J., Quinn, M.J., Richards, W.N. and Wilson, T.S. (1984) ‘Reduction in exposure to lead from drinking water and its effect on blood lead concentrations’, Human Toxicology, 3(5), pp. 383–392.
Sherlock, J., Smart, G., Forbes, G.I., Moore, M.R., Patterson, W.J., Richards, W.N. and Wilson, T.S. (1982) ‘Assessment of lead intakes and dose-response for a population in Ayr exposed to a plumbosolvent water supply’, Human Toxicology, 1(2), pp. 115–122.
Taumata Arowai (2025) Plumbosolvency. Wellington: Water Services Authority.
Taumata Arowai (2026) New rules introduced for lead-free plumbing products. Wellington: Water Services Authority.
Thames Water (2024) PR24 Water Quality: Long Term Water Quality Strategy — Lead (TMS22 Enhancement Case). Reading: Thames Water.
Umweltbundesamt (2023) Dittmann, D. and Janke, N., Abschätzung der in Deutschland noch vorhandenen Bleileitungen. UBA Texte 74/2023. Dessau-Roßlau: Umweltbundesamt.
US EPA (2019) Strategies to Achieve Full Lead Service Line Replacement. Washington, DC: United States Environmental Protection Agency.
US EPA (2023) Seventh Drinking Water Infrastructure Needs Survey and Assessment Report to Congress. Washington, DC: United States Environmental Protection Agency.
US EPA (2024a) National Primary Drinking Water Regulations for Lead and Copper: Improvements. Federal Register.
US EPA (2024b) Lead and Copper Rule Improvements. Washington, DC: United States Environmental Protection Agency.
Watt, G.C.M., Britton, A., Gilmour, W.H., Moore, M.R., Murray, G.D., Robertson, S.J. and Womersley, J. (1996) ‘Is lead in tap water still a public health problem? An observational study in Glasgow’, BMJ, 313(7063), pp. 979–981.
Watt, G.C.M., Britton, A., Gilmour, W.H., Moore, M.R., Murray, G.D. and Robertson, S.J. (2000) ‘Public health implications of new guidelines for lead in drinking water: a case study in an area with historically high water lead levels’, Food and Chemical Toxicology, 38(1), pp. 73–79.
